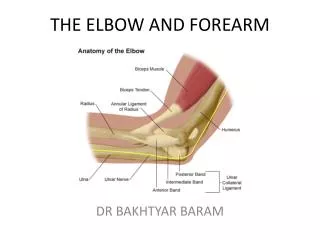
Elbow and forearm
Elbow and forearm. CLASSIFICATION Injuries of the elbow Dislocation of the elbow Dislocation of the head of the radius Subluxation of the head of the radius Contusion of the elbow Fractures of the forearm bones. INJURIES OF THE ELBOW. DISLOCATION OF THE ELBOW

Elbow and forearm
E N D
Presentation Transcript
CLASSIFICATION • Injuries of the elbow • Dislocation of the elbow • Dislocation of the head of the radius • Subluxationof the head of the radius • Contusion of the elbow • Fractures of the forearm bones
INJURIES OF THE ELBOW DISLOCATION OF THE ELBOW Dislocation of the elbow is usually caused by a heavy fall onto the outstretched hand. It is a fairly common injury both in children and in adults. Pathology: The dislocation is nearly always posterior or posterolateral(Fig. 12.1). That is to say, the ulna and the radius are displaced backwards, or backwards and laterally, relative to the humerus. There may be an associated fracture of the coronoid process of the ulna, or of the radial head.
Treatment The dislocation should be reduced under anaesthesia as soon as possible. Reduction is usually easy: all that is necessary is to pull steadily upon the forearm with the elbow semi flexed,while direct pressure is applied behind the olecranon. Reduction should be confirmed by radiographic examination and clinical tests: the radiographs should be scrutinised for one or more of the fractures mentioned above. Thereafter it is recommended that the elbow be rested in a plaster backslap in 90° of flexion for 2 weeks before mobilizing exercises are begun. A plaster affords the best conditions for healing of the injury to the soft tissues, which is often extensive; furthermore, it allows greater freedom of movement at the shoulder and hand than does the collar and cuff sling that is often prescribed for this injury.
Complications 1-Vascular or nerve injury. Occasionally the brachial artery or one of the major nerve trunks is damaged in a dislocation of the elbow, 2-Joint stiffness. The elbow is prone to troublesome stiffness after injury, and especially after dislocation. The stiffness is usually caused by intra-articular and peri-articular adhesions and it will gradually yield to active exercises, provided they are persevered with tor long enough. Manipulation and passive stretching should be avoided: the elbow never lends itself well to manipulation and, indeed, stiffness may often be made worse thereby. 3-A less common but more serious cause of stiffness is post-traumatic ossification (wrongly termed myositis ossificans), a condition in which new bone forms in the haematoma beneath the stripped-up periosteum and joint capsule (Fig. 12.2).
Fig. 12.7 The Monteggia fracture-dislocation, a combination of fracture of the upper half of the ulna with dislocation of the head of the radius. The displacement is usually forwards, as shown here, but the reverse deformity may occur.
FRACTURE OF THE UPPER END OF THE ULNA WITH DISLOCATION OF THE HEAD OF THE RADIUS (Monteggiafracture-dislocation) This uncommon injury is usually caused by a fall associated with forced pronation of the forearm, but a similar injury may be caused by a direct blow on the back of the upper forearm. The usual displacement is characteristic: the distal ulna is angled forwards and the head of the radius is dislocated forwards (Fig. 12.7). Rarely, the reverse deformity occurs. Treatment For this complex injury, accurate reduction is essential and is seldom possible using closed methods, except occasionally in children. operation is normally required to reduce and fix the ulna fracture with a plate and screws. The elbow and forearm should then be immobilized in a plaster cast at a right angle for 4-6 weeks. In the rare event where the postoperative radiograph shows incomplete reduction, an open reduction may be necessary.
FRACTURE OF THE SHAFT OF THE RADIUS WITH DISLOCATION OF THE INFERIOR RADIO-ULNAR JOINT (Galeazzifracture-dislocation) In this injury the shaft of the radius is fractured near the junction of its middle and lowest thirds, the ligaments of the inferior radioulnarjoint are ruptured and the head of the ulna is displaced from the ulnar notch of the radius. The fragments of the radius are usually tilted medially towards the ulna (Fig. 12.12). The injury is analogous to the Monteggia fracture-dislocation in the upper part of the forearm (p. 171): it is said to be more common than the Monteggia injury. The cause is usually a fall onto the hand.
Treatment Perfect reduction is essential for restoration of full function. Only occasionally and then usually in children can adequate reduction be gained and maintained by conservative methods. In adults redisplacement is common after reduction by manual traction and supination, so resort must usually be had to operative reduction and internal fixation of the radial fracture, preferably by a metal plate with screws. The position is held by a full length arm plaster with the elbow flexed to the right angle and the forearm supinated: the plaster is retained until union occurs.
FRACTURE OF THE LOWER END OF THE RADIUS (Colles's fracture) The Colles‘s fracture is seen more often than any other injury in fracture clinics. It is not the most common fracture at all ages indeed, it occurs rather infrequently in young adults but it is certainly the most common fracture in persons over 40 years of age, and especially in women. The association of the fracture with osteoporosis is now well established and it is frequently the first indication of the presence of a generalized loss of bone mass. The condition and its association with the other so called 'fragility fractures‘. The fracture is nearly always caused by a fall onto the outstretched hand.
The typical deformity In a few cases there is simply a crack without displacement, but in the great majority the fracture and displacement are characteristic. The fracture occurs transversely about 2 cm above the lower articular surface of the radius. The lower fragment is displaced slightly backwards and laterally and is tilted backwards, so that the articular surface, instead of pointing downwards and slightly forwards as in the normal wrist, is directed downwards and backwards (Figs 12.13-12.16). The lower fragment is also driven upwards and impacted into the upper fragment. The styloid process of the ulna is commonly detached, but not always. .
This typical displacement is reflected in a characteristic clinical appearance that has been termed the 'dinner-fork' deformity (Fig. 12.14). There is a dorsal hollow or depression in the lowest third of the forearm (proximal to the fracture), but immediately below this there is a marked prominence caused by the lower fragment's being displaced backwards, carrying with it the whole of the carpus and hand. Anteriorly there is fullness where the soft tissues are stretched over the forward projecting upper fragment.
Fig. 12.13 The typical displacement in Colles's fracture. The distal fragment of the radius is tilted backwards so that the articular surface is directed downwards and backwards instead of downwards and slightly forwards as in the normal state. The distal fragment is often also shifted backwards, as depicted here. The normal state is shown for comparison, with the level of the fracture indicated by interrupted line.
Reversed deformity In a small proportion of fractures of the lower end of the radius the deformity is the reverse of that described above. That is, the lower fragment is displaced forwards and rotated forwards so that the articular surface is directed too far anteriorly. This variation, known as Smith's fracture. Treatment In displaced fractures the standard method of treatment is to undertake manipulative reduction under either local or general anaesthesia and to immobilize the forearm and wrist in a below-elbow plaster. In effecting the reduction the fragments must first be disimpactedand the bone drawn out to full length: the distal fragment can then be repositioned accurately by firm pressure over its dorsal surface (see Fig. 12.18). Technique of reduction. The muscles of the forearm should be relaxed, either by general anesthesia (supplemented if necessary by a relaxant) or by regional anesthesia. The first step is to disimpact the fragments, which have often been driven together firmly in the position of deformity.
Fig. 12.15 A typical Colles fracture of the lower end of the radius. Note in the lateral view the backward displacement and backward tilt of the lower fragment, whose articular surface now points downwards and backwards. In this case the styloid process of the ulna is intact: commonly it is fractured near its base.
Fig. 12.16 The fracture seen through plaster after manipulative reduction, Normal alignment is restored. Note in the lateral radiograph that the articular surface of the radius is directed downwards and slightly forwards-the normal orientation.
Fig. 12.17 First step in the reduction of a fracture of the lower end of the radius with backward tilting of the distal fragment: traction is being applied to disimpact the fragments.
In the management of a Colles's fracture it is important that the position of the fragments be checked by radiographs in two planes immediately after the reduction. These radiographs should be repeated at the time of the first check examination, because there is a risk of redispiacement as the soft-tissue swelling subsides, despite immobilization in plaster. If the check radiographs show that redispiacement has occurred, further manipulative reduction under anesthesia should be advised. Usually it is impossible to correct a redispiacement by manipulation if it has been allowed to persist for more than 2 weeks, so it is important to ensure that any redispiacement is detected early.
While the limb is in plaster the patient should be encouraged to use the hand freely for everyday activities, and deliberate exercises should be carried out for the fingers, elbow and shoulder. The plaster should be retained usually for 5-6 weeks, though it may be discarded after 3 or 4 weeks in undisplaced crack fractures. Although union is far from consolidated even at 6 weeks, it is firm enough to ensure that no further displacement will occur, because the leverage acting through the short lower fragment is slight. After the plaster has been removed, a course of mobilizing and muscle strengthening exercises for the wrist and fingers should be arranged.
External fixation. Treatment by an external fixator is increasingly used as an alternative technique in younger patients with severely comminuted or displaced unstable Colles's fractures (Fig. 12.21). A small modified external fixator is required with insertion of the distal pins either into the distal radial fragment.
Internal fixation. In the presence of continued instability or severe comminution, particularly in the younger patient, some surgeons use limited internal fixation of the fragments to stabilize the reduction. After closed reduction into an acceptable position, multiple percutaneous Kirschner wires or pins are inserted under radiographic control to secure the comminuted fragments. Dorsal plate fixation is less suitable for the Colles's fracture as it may interfere with extensor tendon function.
Complications 1-Mal-union 2-Subluxation of the inferior radioulnar joint, 3-Rupture of the tendon of extensor pollicis longus, 4-Compression of the median nerve, 5-Stiffness of the fingers or shoulder from neglected use, and 6-Reflex sympathetic dystrophy (Sudeck's atrophy) of the bones of the wrist and hand.
Fig. 12.23 Transfer of extensor indicis to replace a ruptured extensor pollicis longus. This transfer is preferred to direct suture when the ends of the ruptured tendon are frayed.
FRACTURE OF THE LOWER END OF THE RADIUS WITH ANTERIOR DISPLACEMENT (Smith's fracture, Barton's fracture) in a small proportion of cases fracture of the lower end of the radius is associated not with the typical posterior displacement and posterior tilting of the distal fragment that characterize the Colles's fracture, but with the reverse deformity: the distal fragment is displaced forwards and tilted forwards (Fig. 12.24A). This injury is often termed Smith‘sor Barton‘s fracture or, loosely, reversed Colles's fracture. It is usually caused by a fall onto the back of the hand, which at the time of impact is flexed at the wrist.