Download
1 / 21
260 likes | 1.7k Vues
Injuries to the Elbow and Forearm. Tintinalli Chapter 270. Posterior Elbow Dislocation. Mechanism: FOOSH (fall on an outstretched hand) Clinically: held in 45 degree flexion, prominent posterior olecranon, significant swelling Assess neurovascular status before and after reduction

E N D
Injuries to the Elbow and Forearm Tintinalli Chapter 270
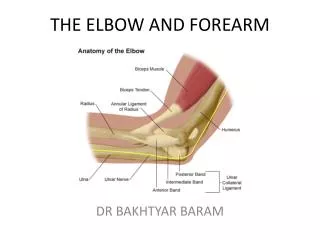
Posterior Elbow Dislocation • Mechanism: FOOSH (fall on an outstretched hand) • Clinically: held in 45 degree flexion, prominent posterior olecranon, significant swelling • Assess neurovascular status before and after reduction • Ulnar, radial, median nerve fxn and brachial artery • X-ray: lateral-ulna & radius displaced posteriorly • Reduce under conscious sedation. Distal traction at wrist with humerus immobilization. Flex the elbow with posterior pressure to the distal humerus. Post reduction films.
Anterior dislocations • Mechanism-elbow flexed with a blow to the olecranon. • Forearm is elongated and supinated • Higher incidence of vascular damage • Reduction: immobilize the humerus with in-line traction to the wrist and downward/backward pressure on the proximal forearm
Radial Head Subluxation • Children<5 y.o. • MOI-longitudinal traction on the hand or forearm with arm in pronation • Presents: elbow flexed and arm in passive pronation, unwilling to move it • Xrays are usually normal • Reduce by placing the thumb on the radial head and supinating the forearm and flexing the elbow
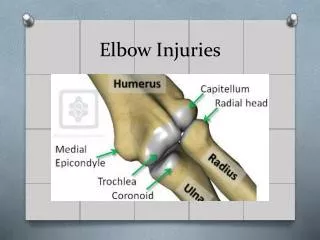
Elbow Radiograph • Post. Fat pad-never normal on x-ray. Represents swelling of the joint capsule and probably fx. • Ant. Fat pad-a small one may be present on normal x ray. If superior and anteriorly displaced, could represent a fracture. • Anterior humeral line-line down the ant. surface of the humerus normally transects the middle of the capitellum. With a supracondylar extension fracture the line may transect the ant. 1/3 or completely ant. to the capitellum
Elbow Radiograph Fat Pad Sign
Supracondylar Extension Fracture • MOI: FOOSH • Clinically: edema, tenderness at elbow, olecranon prominent, depression proximally over triceps • X-ray: Posterior fat pad, tranverse fx line • Treatment • Nondisplaced: ortho consult-post. splint with the arm at 90 degrees • Displaced: require surgical reduction. If vascular compromise, try to reduce once in the ED
Supracondylar Flexion fractures • MOI: direct anterior force against flexed elbow • Xray: anterior displacement of distal fragment (frequently open) • Treatment • Nondisplaced-immobilization with early ortho follow up • Displaced-emergent ortho consult for reduction and pinning
Distal Humerous Fractures • Epicondyle Fractures • Lateral (rare) • Avulsion usually • Immobilize in 90degrees flexion, ortho referral one week • Medial • MOI: repeated valgus (throwing) or direct blow • Presentation: pain over medial elbow worse with supination • Risk: ulnar nerve injury • Tx: nondisplaced – nonoperative; displaced – internal fixation
Distal Humerous Fractures • Condylar fractures • Lateral (more common) • Children • MOI: direct blow, FOOSH, varus stress • Medial • Children • MOI: transmitted force from ulna, FOOSH, valgus • Treatment • Ortho consult for surgical correction
Radial Head Fractures • Most common fx of elbow • MOI: FOOSH • Clinically: pain in lateral elbow with pronation & supination • Xray: • Radiocapitellar line: line drawn from center of radial shaft should transect radial head and capitellum • Abnormal fat pad • Tx • Displaced: surgical • Nondisplaced: sling immobilization, ortho referral 1 week
Olecranon fractures • MOI: direct blow to point of elbow, FOOSH with elbow flexion • Clinically: pain posterior elbow, swelling, crepitus • Triceps function may be compromised • Ulnar N. injury common • Tx • Nondisplaced: immobilize in flexion, forearm neutral • Displaced >2mm ORIF
Forearm Fractures • Radius and ulna: joined by interosseous membrane results in injury to both • Requires high force, MVA, fall from height • Complications: reduced sup/pro, osteo, neurovascular compromise, compartment syndrome, Volkmann’s contracture
Nightstick Fracture • Isolated Ulnar Fracture • MOI: Direct blow to forearm (defensive) • Tx • Nondisplaced: long arm splint, close f/u • Displaced >10 degrees of angulation or >50% of the width: ORIF
Galeazzi fracture • Fracture of distal third of radial shaft with a distal radioulnar dislocation • MOI: FOOSH in forced pronation, direct blow • Xray • Short oblique or tranverse with dorsal lateral angulation • Radioulnar joint injury subtle (increased distal radioulnar joint space on AP view) • Tx: ORIF
Monteggia’s Fracture-Dislocation • Ulnar shaft fx with radial head dislocation • Four Types: • Type I: prox/middle 1/3 ulna, ant dislocation radial head • Type II: prox/middle 1/3 ulna, post dislocation • Type III: fx ulna distal to coronoid process, lateral dislocation • Type IV: prox/middle 1/3 ulna and fx prox 1/3 of radius with ant dislocation
Monteggia Fracture-Dislocation • Clinically • radial head palpable in anterolateral or posterolateral location • Forearm may appear shortened and angulated • Xray • Ulnar fx clearly visible, may overshadow less obvious radial head dislocation • Tx • ORIF of ulna • Closed reduction of radial head dislocation
Biceps Rupture • Proximal (long head) • MOI: repetitive microtrauma (chronic bicipital tenosynovitis), sudden contraction vs resistance • Snap/pop, pain in anterior shoulder, mid arm “ball” • Xray: look for avulsion fx • Tx: sling, ice, analgesics, ortho referral
Triceps Rupture • Rare • Distal more common, young men • MOI: FOOSH causing forceful flexion of extended forearm, direct blow to olecranon • Clinically: sulcus with a more proximal mass, if complete- inability to extend forearm • Xray: look for avulsion of olecranon • Tx: sling, ice, analgesics, ortho referral • Compete tear: surgery • Partial tear: immobilization