Basic Principles of Nutriton
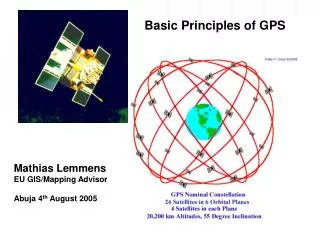
Basic Principles of Nutriton. Prof. Dr. Ahmet AYDIN İÜ Cerrahpaşa Tıp Fak. Çocuk Sağlığı ve Hastalıkları ABD Metabolizma ve Beslenme Bilim Dalı Başkanı (www.beslenmebulteni.com) (besahmet@yahoo.com). NUTRITIONAL REQUIREMENTS.

Basic Principles of Nutriton
E N D
Presentation Transcript
Basic Principles of Nutriton Prof. Dr. Ahmet AYDIN İÜ Cerrahpaşa Tıp Fak. Çocuk Sağlığı ve Hastalıkları ABD Metabolizma ve Beslenme Bilim Dalı Başkanı (www.beslenmebulteni.com) (besahmet@yahoo.com)
NUTRITIONAL REQUIREMENTS • Individual nutritional requirements vary with genetic and metabolic differences. • For infants and children, the basic goals are satisfactory growth and the avoidance of deficiency states. • Good nutrition helps to prevent acute and chronic illness and to develop physical and mental potential; it should also provide reserves for stress.
Oral daily water consumption at various ages Water is essential for existence; a lack of it results in death in a matter of days.
Energy needs • Energy needs of children at different ages and under various conditions vary greatly. • The approximate average expenditures of energy by the child 6-12 yr of age are basal metabolism, 50%; growth, 12%; physical activity, 25%; and fecal loss, about 8%, mainly as unabsorbed fat.
Distribution of calories Approximately • 9-15% of the calories are derived from protein, • 45–55% are derived from carbohydrateand • 35–45% are derived from fat. Each gram of • Ingested protein or carbohydrate provides 4 kcal. • 1 g of long-chain fatty acids provides 9 kcal.
Proteins • Protein constitutes about 20% of adult body weight. Its amino acids are essential nutrients in forming cell protoplasm. • Twenty amino acidshave been identified; eight were found to be essential for children and adults. • Nonessential amino acids can be synthesized and need not be supplied in the diet. • New tissue cannot be formed without all of the essential amino acids simultaneously present in the diet. • The absence or deficiency of only one essential amino acid results in a negative nitrogen balance.
The monosaccharides Glucose Fructose Galactose The disaccharides Lactose: glucose + galactose Sucrose: glucose + fructose Maltose: glucose + glucose The polysaccharides Starch: glucose + glucose + glucose ………. Glycogen: (animal starch) Carbohydrates
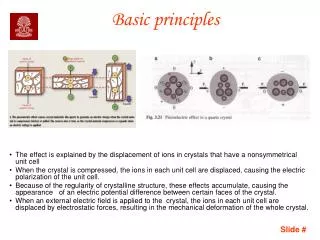
High glycemic load and insulin resistance • Highly refined carbohydrates foods with a high glycemic load and /or index overstimulate insulin secretion. • While hyperinsulinemia causes fat depositon in the fed state, it do not give permission to hydrolysis of fats. • Insulin resistance leads to common chronic diseases.
Glisemik endeksi yüksek rafine gıdaların açlık ve tokluk metabolizması üzerine olan etkileri nelerdir?
KARACİĞER Glikojen KAS Normaltokluk Metabo-lizması İNSÜLİN (+) Yavaş emilen şekerler Glikojen İNSÜLİN (+) Protein İNSÜLİN (+) Trigliserit YAĞ DOKUSU
Normal açlık metabolizması (insülin düşük) KARACİĞER Glikojen GLÜKOZ Protein KAS Hormona duyarlı lipaz Trigliserit YAĞDOKUSU
KARACİĞER Glikojen KAS Glisemik endeksi yüksek gıda alımından sonraki metabo-lizma İnsülin direnci GLÜKOZ Glikojen Protein Trigliserit YAĞ DOKUSU
İnsülin direncinde açlık metabolizması (insülin yüksek) KARACİĞER Glikojen (-) Glikojen GLÜKOZ Protein (-) KAS Trigliserit YAĞDOKUSU Yüksek insülin (-) Hormona duyarlı lipaz
Açlık sırasında, normalde enerjimizin %80’ini veren yağların yeteri kadar yıkılmaması kan şekerini düşürür. • Aşırı şeker alındıktan sonra oluşan bu şeker düşüklüğüne tepkisel (reaktif) hipoglisemidenir. • Reaktif hipoglisemi değişik nöropsikiatrik bulgulara yol açar. Hipoglisemiye giren kişi semptomlarını hafifletmek için şekerli gıdalara aşırı düşer.
Hipoglisemide görülen semptom ve belirtiler Merkezi sinir sistemi depresyonu • Sersemlik • Huzursuzluk • Görme bozukluğu • Garip davranışlar • Başağrısı • Konvülsiyon • Kr. Yorgunluk • Koma Adrenalin artışı • Titreme • Terleme • Çarpını • Halsizlik • Depresyon • Kr. Yorgunluk • Panik atak • Ölüm korkusu
Headaches Multiple sclerosis Alzheimer disease. Hyperactivity Anxiety Depression Concentration difficulties İnappropriate behavior Decreasedperformance Drowsiness Chromium deficiency Copper deficiency Calcium deficiency Magnesium deficiency breast cancer Ovary cancer Gastric cancer Prostate cancer Rectum cancer Colon cancer Gall bladder cancer. Insulin resistance-common chronic diseases I
Reactive hypoglycemia Coronary heart disease Rise in triglycerides Rise in LDL Decrease in HDL Wrinkles Grey hair Baldness Alcoholism Obesity Gallstones Stomach ulcer Appendicitis Fatty liver Crohn's disease Ulcerative colitis Dyspepsia Constipation Bacterial infection Candidiasis Kidney damage Kidney stones Insulin resistance-common chronic diseases II
Arthritis Hemorrhoids Varicose veins Asthma Emphysema Dental caries Periodontal disease Osteoporosis Hypertension Food allergies Diabetes Cataracts Atherosclerosis Free radical formation Fluid retention Myopia Macular degeneration Gout Toxemia (pregnancy) Premensturel syndrome Eczema Insulin resistance-common chronic diseases III
Lipids CH3(CH2)n-COOH Fatty acids G l Cholesterol i s e Esther of Cholesterol r o l Triglycerides G Sfingozin l i s e r o Glükoz/ Fosfat Azotlu baz l Galaktoz Phospholipid Sfingolipi Sphingolipid
ESSENTIAL FATTY ACIDS • Essential fatty acids (EFA) are polyunsaturated and grouped into two families, the omega-6 EFAs and the omega-3 EFAs. • Fats are molecules with a long carbon chain and they have two ends. One end has a methyl group and the other end has a carboxyl group. • The Greek symbol "omega" is used as it is the last letter in the Greek alphabet. When omega is used in reference to fatty acids it is referring to the methyl end of the fatty acid.
Thus Omega-3 fattyacids refer to the family of fatty acids in which the first cis double bond closest to the methyl end of the fat is in the 3rd position. • Omega-6 refers to the family of fatty acids where the first cis double bond closest to the methyl end is in the 6th position.
carboxyl group methylgroup
Although we do need both omega-3s and omega-6s it is becoming increasingly clear that an excess of omega-6 fatty acids can have dire consequences. • Our ancestors evolved on a diet with a ratio of omega-6 to omega-3 of about 1:1. • A massive change in dietary habits over the last few centuries has changed this ratio to >20:1 and this spells trouble.
Sources and requirements • The main sources of omega-6 fats are vegetable oils such as corn oil and soy oil that contain a high proportion of linoleic acid. • Omega-3 fats are found in flaxseed oil, walnut oil, and marine plankton and fatty fish. • The main component of flaxseed and walnut oils is alpha-linolenic acid while the predominant fatty acids found in fatty fish and fish oils are eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA).
Humans do not synthesize linoleic or linolenic acid. Both must be supplied in the diet and are, therefore, "essential." • Linoleic acid is the precursor of arachidonic acid, the prostaglandins and the leukotrienes. • Essential fatty acids are necessary for growth, skin and hair integrity, regulation of cholesterol metabolism, lipotropic activity, decreased platelet adhesiveness, and reproduction.
Tissue phospholipids Dietary omega-6s Fosfolipase A2 Archidonic acid Lipooxigenase Cyclooxigenase (-) (-) Dietary omega-3’s Prostaglandin H2 Leukotiriene A4 Hydrolase Thrombaxane A2 Leukotiriene B4 Prostaglandin E2 Inflamatory mediators
Tissue phospholipids Dietary omega-3s Fosfolipase A2 Eicosapentoenoic acid Lipooxigenase Cyclooxigenase (-) (-) Dietary omega-6’s Prostaglandin H3 Leukotiriene A5 Hydrolase Thrombaxane A3 Leukotiriene B5 Prostaglandin E3 Antiinflamatory mediators
Inflamation Omega-3 Dehydroepiandrosterone Vitamin K Vitamin E n-acetyl cystein Nettle seed Vitamin D (-) cytokines TNF-α interleukine-1(b) interleukine -6
Acne Psychiatric Disorders AIDS Allergies Alzheimer Angina pectoris Atherosclerosis Arthritis Behavioral disorders Senility Immunedeficiency Heart disease Cancer Cystic fibrosis Learning disorders Leukemia Lupus Malnutrition Menopause Schizophrenia Diseases related to omega-3 fatty acids deficiency
Diabetes Dermatitis Infection Inflamatory Diseases Breast Cancer Breast cyst Palsy Vision disorders Hypertension Hyperactivity Metastasis Multipl Sclerose Otoimmunity Obesity Chronic fatigue syndrome Psoriasis Reye syndrome Diseases related to omega-3 fatty acids deficiency
Saturated fatty acids Butter Beef tallow Margarine Monounsaturated fatty acids (omega-9) Olive oil Hazelnut oil Fatty acids Poliunsaturated fatty acids (omega-3) Fish / liver oil Flaxseed oil Wall nut oil Canola oil Poliunsaturated fatty acids (omega-6) Corn Sun flower Soya Cotton
Minerals • Macrominerals. Minerals in which the requirements are over 50 mg/day for an adult. • The principal macrominerals are cations such as calcium, magnesium, potassium, and sodium and their comparable anions are phosphorus, sulfur, and chloride. • Microminerals: Minerals in which the requirements are below 50 mg/day for an adult. • Iron, iodine, and cobalt appear in important organic complexes. The trace elements fluorine, copper, zinc, chromium, manganese, selenium, and molybdenum have known metabolic roles; silicon, boron, nickel, aluminum, arsenic, bromine, and strontium are toxic and also present in the diet and in the body.
B complex vitamins are coenzymes of enzymatic reactions. B complex vitamins that have roles in energy metabolism Vitamin B1 (thiamin) Vitamin B2 (riboflavin) Vitamin B3 (Niacin= nicotinic acid) Vitamin B5 (pantothenic acid) Biotin Other B complex vitamins B12 vitamini (cyanocobalamin) Folic acid Vitamin B6 (pyridoxine) II. Vitamin C (antioxidant) Fat soluble vitamins Vitamin A (antioxidant) Vitamin E (antioxidant) Vitamin D (calcium metabolism) Vitamin K (coagulation) Water and fat soluble vitamins
Water soluble vitamins • Because of their water solubility, excesses of these vitamins are excreted in urine and so rarely accumulate in toxic concentrations. • They are heat-labile and can be absorbed in malabsorption syndromes. Fat soluble vitamins • Because of their fat solubility, excesses of these vitamins are not excreted in urine and accumulate in toxic concentrations. • They are heat-resistant and can not be absorbed in malabsorption syndromes.