Musculoskeletal System
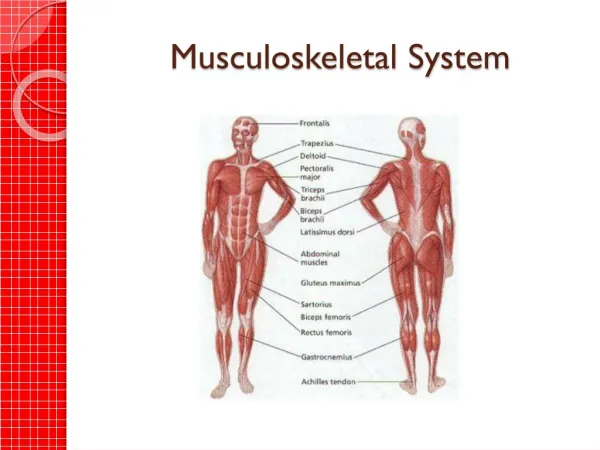
Musculoskeletal System. Introduction. - its consist of bon ’ s, joints& muscles Functions: 1- support to stand erect 2- For movement 3- encase & protect inner vital organs (brain, spinal cord, heart) 4- produce RBC in bone marrow (hematopoiesis)

Musculoskeletal System
E N D
Presentation Transcript
Introduction • - its consist of bon’s, joints& muscles • Functions: • 1- support to stand erect • 2- For movement • 3- encase & protect inner vital organs (brain, spinal cord, heart) • 4- produce RBC in bone marrow (hematopoiesis) • 5- a reservoir for storage essential minerals as Ca & Ph in bones
Component of M.S system • Skeleton is the bony framework of body , it has 206 bones, bone hard, continually turnover . Joints is the place of union of 2 or more bones, its permit permeability. • Nonsynovial or Synovial Joints: • In non Synovial joints bones are united by fibrous tissue or cartilage & immovable (vertebra). Synovial joints frely movable, cavity filled with a lubricant or synovial fluid.
It has a layer of cartilage covers the surface of opposing bones, cushions the bones & gives a smooth surface to facilitate movement. • Joints surrounded by ligaments. • Muscles: 40-50% of body weight, when they contract produce movement. • 3 types: skeletal, smooth, cardiac.skeletal is voluntary muscles.
Skeletal muscles are attached to bones by a tendon: producing the following movements: 1- flexion: bending a limb at a joint 2- Extension: straightening a limb at a joint 3- Abduction: moving a limb away from midline 4- Adduction: moving a limb toward midline.
5- pronation: turning the forearm so that palm is down • 6- Supination: turning forearm so palm up. • 7- Circumduction: moving arm in a circle around the shoulder • 8- Inversion: moving sole of foot inward at ankle • 9- Eversion: moving sole of foot outward at ankle 10- Rotation: moving head around a central axis
11- protraction: moving a body part forward & parallel to ground. 12- Retraction: moving a body part backward& parallel to ground. 13- Elevation: raising a body part 14- Depression: lowering a body part.
Landmarks • Temporomandibular joint: articulation of mandible & temporal bone • Spine: • 1- C7& T1 prominent • 2- inferior angle of scapula between T7& T8. • 3- line of iliac crest crosses L4 • 4- line of posterior iliac spines crosses sacrum
Shoulder: 1- acromion process; at the top of shoulder 2- greater tubercle of humerus • Elbow: 1- medial & lateral epicondyles of humerus 2- olecranon process of ulna • Wrist & carpals: • 1- radiocarpal joint: articulation of radius & a row of carpal bones permit flexion& extension& side to side deviation • 2- midcarpal joint : between 2 rows of carpal bones. Allows flexion , extension & rotation
3- metacarpophalangeal & interphalangeal joints permit finger flexion & extension • Hip: 1-anterior superior iliac spine2- ischial tuberosity. 3- greater trochanter of femur • Knee: 1-quadriceps muscle 2- tibial tuberosity • Ankle & Foot: medial & lateral malleolus
Subjective Data: • 1) Joints: pain-stiffness-swelling-heat-redness-limitation of movement • 2)muscles: pain (cramps)- weakness • 3) bones: pain- deformity- trauma • 4) functional assessment (ADL): bathing- toileting -grooming-eating…..etc • 5) self care behaviors
Objective Data: • * preparation: 1- make him comfortable before & throughout exam • 2- take an orderly approach _head to toe, proximal to distal • 3- joints examined should be supported at rest • 4- use firm support gentle movement & return to a relaxed • 5- compare corresponding paired joints (symmetry)
Order of exam • *Inspection; note the size& contour of joint, inspect skin for color, swelling, masses or deformity • * Palpation: palpate each joint, skin, muscles, note the heat, tenderness, swelling or masses • * ROM: range of motion: • Ask for active ROM if you see a limitation attempt passive motion.
Muscle testing • Test the strength of muscle for each joint ask person to flex& hold as you apply opposing force. • Slide table 22-2 page 616
Temporomandibular joint: • Inspect area anterior to ear, place tips of your first 2 fingers in front of each ear & ask person to open & close mouth. an audible & palpable click occur normally. • Palpate contracted temporalis & masseter muscles as person clenches teeth. Compare Rt & Lt for size, strength. Ask him to move the jaw forward & laterally against your resistance & to open mouth against your resistance (CN V)
Cervical spine: • Inspect alignment of head & neck .should be straight & head erect • Palpate spinous processes & sternomastoid, trapezius& paravertebral muscles, should feel firm, no spasm or tenderness, ask him to follow the motions: • Extension -flexion • Lateral bending • Rotation Repeat motions while applying opposing force( CN XI)
Upper Extremities: shoulder • Inspect & compare both shoulders post &ant. • Check size & contour of joint & compare shoulders for equality of bony landmarks, normally no redness, muscular atrophy, deformity or swelling. • If reports pain, ask to point spot, it may from local causes or referred pain to hiatal hernia or cardiac or pleural condition • Palpate both shoulders noting any muscular spasm or atrophy, swelling, heat, or tenderness.
shoulders • Start at clavicle then acromioclavicular joint, scapula, greater tubercle of humerus& glenohumeral joint. • Palpate axilla no adenopathy or masses . • Test ROM; • Forward flexion -hyperextension • Abduction-adduction • Internal rotation • External rotation • Test the strength of shoulder muscles, ask him to shrug shoulders flex forward &up. abduct against your resistance (CN XI)
Elbow • Inspect size & contour of elbow in both flexed & extended positions. Look for deformity, redness or swelling. Check olecranon bursa • Palpate with elbow flexed about 70 degrees & relaxed as possible, use Lt hand to support Lt forearm & palpate olecranon process & medial & lateral epicondyles of humerus, with Rt thumb& fingers in medial groove, normally feel fairly solid, check for synovial thickening, swelling, nodules or tenderness. • Palpate for heat, swelling, tenderness or nodules.
ROM • Flexion -extension • Pronation - supination • Test muscle strength: flex elbow against your resistance, then ask him to extend elbow against your resistance.
Wrist & hand: • Inspect on dorsal & palmar sides, noting position, contour& shape. Normal position shows wrist in slight extension. Fingers lie straight in same axis a forearm, no swelling or redness, deformity or nodules. • Skin smooth with knuckle wrinkle present & no swelling or lesions. • Palpate joint in wrist & hands, support hand with your fingers under it & palpate the wrist firmly with both your thumbs on its dorsum. Move your palpating thumbs side to side to identify the normal depressed areas that overlie the joint space normally feel smooth, no swelling, nodules or tenderness
Palpate metacarpopharyngeal joints with your thumbs. use your thumb& index finger in a pinching motion to palpate the sides of interphangeal joints. Normally no synovial thickening, tenderness, warmth, or nodules • ROM: Extension -flexion • Hyperextension- flexion • Ulnar deviation- radial deviation • Test muscle strength: position forearm supinated on table, stabilize by holding your hand at the person’s midforarm. ask to flex wrist against your resistance at the palm.
Phalen’s test: • Ask person to hold both hands back while flexing wrists 90 degrees, acute flexion of wrist for 60 seconds produce no symptoms normally. • TINEL’S SIGN: • Direct percussion of the location of median nerve at the wrist produces no symptoms normally.
Lower Extremity: • HIP: • Inspect symmetric levels of iliac crests, gluteal folds& equally sized buttocks, even gait reflects equal leg lengths & functional hip motion. • Palpate hip joints (supine position), should feel stable & symmetric, no tenderness or crepitance.
ROM • Extension – hip flexion with knee straight • Extension- hip flexion with knee flexed • External rotation- Internal rotation • Abduction - Adduction
Knee: inspection • Remain Supine with leg extended, or flex knee & dangling for inspection, skin normally looks smooth, even , no lesions. • Lower leg should extend in same axis as thigh. • Inspect knee’s shape & contour. Normally hollows present on either side of patella, check for swelling, check quadriceps muscle in anterior thigh for atrophy its important for joint stability during weight –bearing.
palpation • (supine position), start on anterior thigh,10 cm above patella, palpate with your Lt thumb & fingers in a grasping fashion, exploring supra patellar pouch. Note consistency of tissues. Muscles & soft tissues feel solid& joint should feel smooth, no warmth, tenderness, thickening, or nodularity. When swelling occurs, to distinguish between tissues swellings or fluids in joints, use the 2 tests:
Bulge Sign: • Confirms presence of small amounts of fluid. • Firmly stroke up on medial aspect of knee 2 or 3 times to displace any fluid. • Tap lateral aspect, watch medial side in hollow for a distinct bulge from a fluid wave, normally none is present.
Ballottement of Patella: • Reliable when larger amounts of fluid are present. Use your Lt hand to compress the suprapatellar pouch to move any fluid into knee joint. With your Rt hand, push patella sharply against the femur. If no fluid is present the patella is already snug against femur. • Continue palpation & explore tibiofemoral joint, check for crepitus by holding your hand on patella as knee is flexed & extended.
ROM: • Extension – Hyperextension – flexion • Check muscle strength by asking to maintain knee while you oppose by trying to pull leg forward. Muscle extension rising from a seated position or squatting.