Download
1 / 36
360 likes | 602 Vues
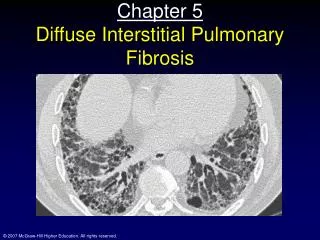
Draft guideline for scoring and reporting interstitial fibrosis. Working Group on Fibrosis Banff 09. Colvin RB B a nff 2009. Rationale. Interstitial fibrosis correlates with function and prognosis in many studies of native and transplant kidneys

E N D
Draft guideline for scoring and reporting interstitial fibrosis Working Group on Fibrosis Banff 09 Colvin RB Banff 2009
Rationale • Interstitial fibrosis correlates with function and prognosis in many studies of native and transplant kidneys • Reproducibility of pathology assessment of fibrosis is modest at best • Definitions and methodology are variable • Fibrosis is an endpoint in some clinical trials and a potential surrogate marker of efficacy Colvin RB Banff 2009
Purpose • Promote more uniform reporting of interstitial fibrosis, quantitation and reproducibility for routine use and clinical trials Colvin RB Banff 2009
Method • Survey pathologists and nephrologists on current practice • Develop guidelines based on these practices and discussion • Validate recommendations Colvin RB Banff 2009
Banff Fibrosis Survey Results 7/22/09-8/11/09 Nephnppt/RPS/WGN Colvin RB Banff 2009
Mostly pathologists 201 Completed survey 96% of those completed form were pathologists Colvin RB Banff 2009
Trichrome most common (97% Masson) Other stains often used in conjunction with trichrome Colvin RB Banff 2009
Important heterogeneity in definition Those using % area more commonly had morphometry access (59% vs 41%) Colvin RB Banff 2009
Banff definition of fibrosis scores (ci) Grade I (mild) Mild interstitial fibrosis and tubular atrophy (<25% of cortical area) Grade II (moderate) Moderate interstitial fibrosis and tubular atrophy (26-50% of cortical area) Grade III (severe) Severe interstitial fibrosis and tubular atrophy/loss (>50% of cortical area) Is mild but diffuse (>50%) fibrosis ci3?
Most score at low power, overall appearance (69%) Colvin RB Banff 2009
Usual exclusions: normal perivascular tissue, subcapsular cortex Colvin RB Banff 2009
Marked heterogeneity in what should be included Colvin RB Banff 2009
Varied consideration of TA in assessment of fibrosis Colvin RB Banff 2009
Confusion on the definition of ci 1 <50% got the correct answer (6-25) Colvin RB Banff 2009
Majority report % fibrosis (65%) Many report ci score (42%) Colvin RB Banff 2009
Pattern but not activity commonly reported Colvin RB Banff 2009
Cellularity most common measure of activity Colvin RB Banff 2009
Visual Trichrome most common for routine use (76%) Colvin RB Banff 2009
Morphometry is a research (64%) not a clinical tool (3%) Colvin RB Banff 2009
DRAFT RECOMMENDATIONS FOR SCORING AND REPORTING FIBROSIS Fibrosis is defined as abnormal accumulation of fibrillar collagen and associated matrix proteins in the cortical interstitium Colvin RB Banff 2009
ROUTINE PRACTICE Scoring Stain: Trichrome (Masson) (+PAS/H&E/silver) Thickness: 2-4 microns Assessment: Global low power (4-10x), Alternate: Average 20x fields Definition of area: % of cortex affected by fibrosis, Alternate: % area of cortical fibrous tissue by morphometry Include: Cortical interstitium of cortex bounded by glomeruli Areas of tubular loss with minimal fibrosis Periglomerular fibrosis Exclude: Subcapsular cortex Normal fibrous tissue around arteries Areas with inflammation without fibrosis Colvin RB Banff 2009
Reporting Extent: % fibrosis to nearest 5% (or 10%) + Banff ci Pattern: Focal, multifocal, diffuse other terms (to be defined): Loose, dense, striped, periglomerular, subcapsular… Activity: Presence of mononuclear infiltrate in fibrotic areas Evolution: Note comparison with last prior biopsy Normal cortex: % of cortex without fibrosis or tubular atrophy Colvin RB Banff 2009
Guide for scoring interstitial fibrosis in renal biopsies C. Bellamy, Edinburgh Colvin RB Banff 2009
VALIDATION • Recommended visual scoring method will be validated by an open multicenter trial • ~30 biopsies evaluated in scanned whole slides. • Participation open (Banff, RPS, WGN pathologists). • Will include transplant and native kidney biopsies. Colvin RB Banff 2009
VALIDATION • Virtual slides (Trichrome and PAS) hosted on a web site in Edmonton • Two phases: a training set and a validation set of 10 and 30 cases, respectively • Scores will be entered via the ”Surveymonkey” system used for the fibrosis survey • Other centers are encouraged to provide a few cases each (either as Aperio scans or by sending slides to Michael Mengel to be scanned in Edmonton) • Cases will be presented with a trichrome and a PAS, at least 7 glomeruli (two cores preferred but not necessary. Native or transplant biopsy, with a wide range of fibrosis (0-100%).
2-4 micron sections most common (90%) Colvin RB Banff 2009
Confusion on what IF/TA score means ?Sum of ci and ct ?Average ci and ct ?Higher of ci or ct Colvin RB Banff 2009 Colvin RB Banff 2009
Highly variable maximum Those using morphometry % area less Colvin RB Banff 2009
Maximum varies by definition of fibrosis area % cortical area (~morphometry) % involved cortex 41% Access to morph facilities 59% Colvin RB Banff 2009
5% most common as upper limit of normal Colvin RB Banff 2009
Clinical trials -visual and morphometry trichrome rec. Colvin RB Banff 2009
Morphometry available to a minority (47%) Colvin RB Banff 2009
Trichrome is most common (42%) for morphometry Sirius red and collagen III also used Colvin RB Banff 2009
CLINICAL TRIALS Visual score As routine, plus Morphometry At least one technique: Trichrome Sirius red Collagen III Colvin RB Banff 2009
Range expected: Maximum 100% (less with morph method). <5% = normal Normal cortex: Score % of cortex without fibrosis or tubular atrophy Colvin RB Banff 2009