Download
1 / 35
350 likes | 363 Vues
Explore the theories, interventions, and reinforcement strategies in addiction treatment protocols based on research by experts like John Marsden and B.F. Skinner. Discover the impact of voucher-based incentives on treatment compliance and relapse rates, with insights from clinical studies on varying treatment protocols and outcomes. Uncover how cognitive-behavioral therapies and contingency management strategies contribute to sustained cocaine abstinence in addiction recovery programs. Evaluate the effectiveness of combining therapies and addressing key issues for future directions in addiction treatment research.

E N D
How much would it cost me to buy a day’s abstinence? Behaviour therapies in the addictions John Marsden, Ph.D. Division of Psychological Medicine & Psychiatry National Addiction Centre, King’s College London, UK
“Failure” Rates for Addictions(reduction <50% in use after 6 mos.) O’Brien & McLellan, 1996, The Lancet
Comparative Rates for Treatment Compliance & Relapse O’Brien & McLellan, 1996, The Lancet
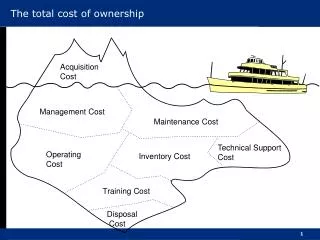
Behavioural interventions • Theoretical foundations • Laboratory and clinical foundations • Reinforcement …. a process wherein a stimulus event increases the future probability of drug use by acting as a consequence. • Effective interventions • Combination therapies • Key issues and future directions
B.F. Skinner • Three-term contingency • Discriminative stimulus • Operant response • Reinforcement (positive and negative) • Behaviour modified by consequences • Schedules of reinforcement • Drug self-adminstration at the core • Drugs function as primary reinforcers • Altering behavioural contingencies
Laboratory Foundations (1) • Opiates, psychostimulants, nicotine, alcohol and cannabis serve as reinforcers in a diverse range of species • Behaviours aimed at obtaining drugs exhibit strong motivational pressure • Animal drug use can be modified by manipulating variables that affect other operant behaviours: • Increasing number of responses required • By blocking/eliminating the reinforcement • By punishing the responses on which drug reinforcement is contingent
Laboratory Foundations (2) • Associative learning and memory processes underpin addiction
Treatment Protocol • Weeks 1-12 • 2x weekly counseling • 3x weekly urine testing • Weeks 13-24 • 1x weekly counseling • 2x weekly urine testing • Months 7-12 • Aftercare – 1x monthly check-in with counsellor • Random urine testing Elements: • Antabuse therapy (clinical punishment) • Relationship counseling & skills training • Occupational assistance • Vouchers for goods and services
Vouchers (weeks 1-12 only) • Urine tests negative for benzoylecgoine (BE) earned points worth $0.25. • The first BE negative earns 10 pts @ $0.25 • Voucher for each subsequent consecutive negative test increases by 5 pts. • The equivalent of $10 bonus is earned for every 3 consecutive negative tests.
Voucher protocol • BE-positive tests or failure to give a specimen ‘reset’ vouchers back to initial value. • BE-positive tests or failure to give a specimen reset vouchers back to initial value. • 5 consecutive negative tests returned vouchers back to the value preceding a reset. • Vouchers were exchangeable for retail items in community; max. earnings possible = $997.50 • All purchases were made by staff and had to be deemed by therapists to be recovery appropriate.
Higgins et al. (1994) Incentives Improve Outcome in Outpatient Behavioral Treatment of Cocaine Dependence. Arch. Gen. Psychiat, 51, 568-76 • 40 patients randomlized to two groups • Treatment lasts for 25 weeks. • 2x weekly counseling and 3x weekly urinalysis in weeks 1-12; reduced to 1x weekly counseling and 2x weekly urinalysis in weeks 13-24. • Counseling in both groups based on the Community Reinforcement Approach (CRA). • Voucher group rewarded for BE-negative results in weeks 1-12. During weeks 13-24, both groups received only a single $1 lottery ticket for each BE-negative test.
Higgins et al. (2000) Contingent Reinforcement Increases Cocaine Abstinence During Outpatient Treatment and 1 Year of Follow-up. JCCP, 2000, 68, 64-72 • 70 patients randomized to two groups. • Treatment over 24 weeks and 1 year follow-up • All get CRA + vouchers • One group receives vouchers contingent on cocaine abstinence • Other group receives vouchers non-contingently (yoked control) • 24 weeks treatment and 1 year of follow-up
Iguchi et al. (1997) Reinforcing operants other than abstinence in drug abuse treatment. JCCP, 65, 425- • 103 MMT patients who completed 6 weeks of baseline testing to one of three conditions: (a) standard MMT (b) MMT + up to $15/week in vouchers for submitting drug-free urine samples (c) MMT + up to $15/week in vouchers for submitting treatment plan tasks • Interventions over 12 weeks • Follow-up over 6 months
TP Interventionhas greater time effect that other 2 treatmernts % drug-free urine samples
Epstein et al. (2003) Cognitive–Behavioral Therapy Plus Contingency Management for Cocaine Use: Findings During Treatment and Across 12-Month Follow-Up. Psychol Addict Behav; 17, 73–82. • 193 MMT outpatients randomized tovoucher availability (contingent or not contingent on cocaine-negative urine testing. • Follow-ups at 3, 6 and 12 months
A meta-analysis of voucher-based reinforcement therapy for substance use disorders. Jennifer Lussier et al. (2006) Addiction, 101, 192-203
Methods • Effect sizes calculated for controlled studies VBRT published between 1/91 & 3/04 • 65 studies reviewed, including 40 where effects of contingent vouchers were experimentally isolated • Focus was on period when vouchers were available • Studies grouped by moderator variables: type of drug targeted, control, duration of VBRT, voucher $ value, voucher delivery immediate or delayed, study setting
Experimental vs control conditions • Results as pearson correlation coefficient where as a guide: r = 0.10 (difference in effectiveness of 55% vs. 45%) r = 0.30 (65% vs. 35%) r = 0.50 ( 75% vs. 25%) • 65 studies reviewed, including 40 where effects of contingent vouchers were experimentally isolated • Studies grouped by moderator variables: type of drug targeted, control, duration of VBRT, voucher $ value, voucher delivery immediate or delayed, study setting
Lambeth Harbour Study • Randomised controlled trial • Voucher-CM only • Synergistic voucher-CM + group based CBT • 82 service users (primary cocaine) • 8 week intervention • 3 x weekly on-site, urine testing for cocaine • 8 x 1.25 hr CBT with CM discussion focus • All participants receive 8 x 1 hr keworking • Follow-ups: • At 1-month (week 12) • At 3-months (week 24)
Outcome criteria • (1) Immediate abstinence during weeks 7 & 8. Participants must provide at least 2 cocaine negative urine tests in each of weeks 7 and 8 and no positive tests. • (2) Short-term abstinence no reported use of cocaine during weeks 9-12 and provision of a negative urine test at the 12-week (1-month) follow-up; and • (3) Longer-term abstinence no reported use of cocaine during weeks 21-24 and provision of a negative urine test at the 3-month follow-up. Statistical analysis by relative risk ratios for outcome criteria and NNT
Lambeth voucher-CM • 24 tests on Monday, Wednesday & Friday • Escalating schedule starting at £1 • Up by £0.5 for each successive –ive test • Bonus for each series of 6 –ive tests • Re-set following +ive test or DNA • Return to previous level for 6 –ives (if time) • Voucher for attending drop-in for 1.25 hours • Final bonus for attending for all 24 tests • Total voucher value possible = £323 • Harbour voucher credits exchanged for store gift certificates as Argos, Footlocker, Woolworths etc.
The Harbour Steps 12 11 10 9 8 7 6 5 4 3 2 1 Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Week 8
Lambeth CBT • All CBT attenders receive CM • CBT has joint CM coaching and CBT skills training purpose • Key themes: • Showing you the ropes • The CM rules! • Clearance reassurance • Personal voucher goals • Getting rolling • Brushing off a set-back • The crunch zone • Helping others • CBT skills
Key issues and future directions • Behavioural interventions using CM are effective at encouraging initial abstinence. • When contingencies removed effects taper off. • However, they are rarely used in routine treatment delivery settings and outside the USA. • They may be particularly effective when combined/integrated with other interventions. • Further development of reinforcement schedules is needed: non-abstinent reinforcement as initial step?