Successful Treatment of Infantile Onychomycosis with 5% Amorolfine Nail Lacquer
Onychomycosis is among the most common nail disorders, and its prevalence increases with age. This case details a 16-month-old boy with superficial white onychomycosis (SWO), linked to a family history of the infection. Standard antifungal treatments are not officially approved for infants, making this case noteworthy. Diagnosed through KOH examination and fungal culture, the infant was effectively treated with 5% amorolfine nail lacquer with no side effects. After a structured treatment plan lasting six months, the child showed complete cure and no recurrence upon follow-up.

Successful Treatment of Infantile Onychomycosis with 5% Amorolfine Nail Lacquer
E N D
Presentation Transcript
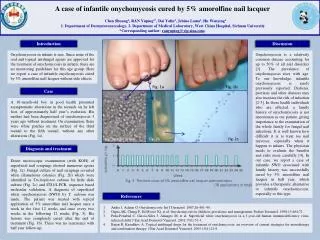
Introduction Discussion Onychomycosis is a relatively common disease accounting for up to 50% of all nail disorders [1]. The prevalence of onychomycosis rises with age. To our knowledge, infantile onychomycosis is rarely previously reported. Diabetes, psoriasis and other diseases may also increase the risk of infection [2-3]. In those health individuals who are affected, a family history of onychomycosis is not uncommon as our patient, giving importance to the examination of the whole family for fungal nail infections. It is well known how difficult it is to treat toe nail mycoses, especially when it happen to infants. The physician needs to evaluate the benefits and risks more carefully [4]. In our case, we report a case of infantile SWO associated with family history was successfully cured by 5% amorolfine nail lacquer in half year, which provides a therapeutic alternative to infantile onychomycosis, especially to this type. A case of infantile onychomycosis cured by 5% amorolfine nail lacquerChen Shuang1, RAN Yuping1*, Dai Yalin2, Jebina Lama1,Hu Wenying11. Department of Dermatovenereology, 2. Department of Medical Laboratory, West China Hospital, Sichuan University*Corresponding author: ranyuping@vip.sina.com. Fig. 1a Fig. 1b Case A 16-month-old boy in good health presented asymptomatic alterations in the toenails on he left foot, of approximately half year’s evolution. His mother had been diagnosised of onychomycosis 3 years ago without treatment. On examination, there were white patches on the surface of the third toenail to the fifth toenail, without any other alterations (Fig. 1a). Fig. 2a KOH ×400 Fig. 2b Fig. 2c Onychomycosis in infants is rare. Since none of the oral and topical antifungal agents are approved for the treatment of onychomycosis in infants, there are no monitoring guidelines for this age group. Here we report a case of infantile onychomycosis cured by 5% amorolfine nail lacquer without side effects. Diagnosis and treatment Direct microscopic examination (with KOH) of superficial nail scrapings showed numerous spores (Fig. 2a). Fungal culture of nail scrapings revealed white filamentous colonies (Fig. 2b) which were identified as Trichophytonrubrum by little slide culture (Fig. 2c) and ITS1/4-PCR, sequence based molecular validation. A diagnosis of superficial white onychomycosis (SWO) by T. rubrum was made. The patient was treated with topical application of 5% amorolfine nail lacquer once a week in the first 12 weeks and once every two weeks in the following 12 weeks (Fig. 3). His lesions was completely cured after the end of treatment (Fig. 1b). There was no recurrence with half year follow-up. No. of treatment Week Fig. 3 The time cross of 5% amorolfine nail lacquer administration (18 applications in total) References Andre J, Achten G. Onychomycosis. Int J Dermatol. 1987;26:481–90. Gupta AK, Chang P, Del Rosso JQ, et al. Onychomycosis in children: prevalence and management. PediatrDermatol. 1998;15:464-71. Peña-Penabad C, García-Silva J, Almagro M, et al. Superficial white onychomycosis in a 3-year-old human immunodeficiency virus-infected child. J EurAcadDermatolVenereol. 2001;15(1):51-3. Baran R, Kaoukhov A. Topical antifungal drugs for the treatment of onychomycosis: an overview of current strategies for monotherapy and combination therapy. J EurAcadDermatolVenereol. 2005;19(1):21-9.