Download
1 / 11
110 likes | 219 Vues
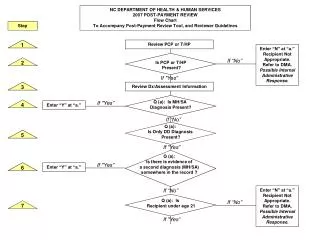
NC DEPARTMENT OF HEALTH & HUMAN SERVICES 2007 POST-PAYMENT REVIEW Flow Chart To Accompany Post-Payment Review Tool, and Reviewer Guidelines. Step. 1. Review PCP or T/HP. Enter “N” at “a.” Recipient Not Appropriate. Refer to DMA. Possible Internal Administrative Response. If “No”. 2.

E N D
NC DEPARTMENT OF HEALTH & HUMAN SERVICES 2007 POST-PAYMENT REVIEW Flow Chart To Accompany Post-Payment Review Tool, and Reviewer Guidelines Step 1 Review PCP or T/HP Enter “N” at “a.” Recipient Not Appropriate. Refer to DMA. Possible Internal Administrative Response. If “No” 2 Is PCP or T/HP Present? If "Yes” 3 Review Dx/Assessment Information Q (a): Is MH/SA Diagnosis Present? If "Yes” 4 Enter “Y” at “a.” If “No” Q (a): Is Only DD Diagnosis Present? 5 If "Yes” Q (a): Is there is evidence of a second diagnosis (MH/SA) somewhere in the record ? If "Yes” 6 Enter “Y” at “a.” If “No” Enter “N” at “a.” Recipient Not Appropriate. Refer to DMA. Possible Internal Administrative Response. Q (a): Is Recipient under age 21 If “No” 7 If "Yes”
Enter “N” at “a.” Recipient Not Appropriate. Refer to DMA. Q (a): Is EPSDT Referral/Approval Present? If "Yes” If “No” 8 Enter “Y” at “a.” Enter “N” at “b”. Training in PCP required. Q (b): Do Dx/Assessments reflect DX Information? If “No” 9 If "Yes” Enter “N” at “b.” Training in PCP required. Q (b): Did Recommended referrals take place? 10 If “No” If "Yes” Q (b): Were recommended consultations related to accurate Dx/assessment information? Enter “N” at “b.” Training in PCP required. If "Yes” If “No” 11 Enter “Y” at “b.” Review the recommendations made on the Summary of Assessments and Observations page of the PCP, or in treatment team notes for a T/HP 12 Enter “N” at “c.” Training in PCP required. Possible Internal Administrative Response. Q (c): Do recommendations reflect DX Information? If “No” If "Yes” 13 Enter “Y” at “c.” Review Symptoms/Observations listed on the Summary of Assessments and Observations page of the PCP or in assessment information for a T/HP. 14
Enter “N” at “d.” Training in PCP required. Q (d): Are they actual symptoms/ Observations? If “No” 15 If "Yes” Enter “N” at “d.” Training in PCP required. Q (d): Do symptoms/observations relate To DX Information? If "Yes” If “No” 16 Enter “Y” at “d.” 17 Review Full Dx/Assessment Information from Q. a-d. Recipient Not Appropriate. Refer to DMA. Possible Internal Administrative Response. If "Yes” Are b-d all rated “N”? 18 Review Personal and Family Interview sections of the PCP. 19 Review Signature page of the PCP or T/HP and/or revisions. 20 Is recipient under age 21? If “No” Is recipient own LRP? 21 If "Yes” If “No” Review participation and agreement of the parent or legally responsible party. 22 Review PCP for family participation, if families identified as participants by individual. 23
Q (e): Did person/family or LRP participated in the development of the plan? Enter “N” at “e.” Training in PCP required. If "Yes” If “No” Enter “Y” at “e.” 24 Review Goal Statements in PCP or T/HP. 25 Q (f): In PCP, is there a symptom/ observation With each goal? If "Yes” 26 If “No” Q (f): In T/HP, Is symptom/observation evident with each goal? Enter “N” at “e.” Training in PCP required. If “No” 27 Enter “N” at “e.” Training in PCP required. Q (f): Do symptoms and observations directly relate to goals? If "Yes” If “No” Enter “Y” at “f.” 28 Review the Personal and Family interview sections in the PCP for comparison to the goal statements to determine if the “What’s Important” information is reflected in the goals. 29 Q (g): In PCP, is the “What’s Important” information reflected in the goals? If "Yes” 30 Enter “Y” at “g.” If “No”
Q (g): If T/HP, do admissions assessments, NC-TOPPS, etc., indicate what is important to individual/family? Enter “N” at “h.” Training in PCP required. If "Yes” If “No” 31 Enter “Y” at “g.” Review the goal statements and supporting interventions in the PCP or T/HP against the appropriate CS Service Definition (Child/Adult/Team). 32 Proceed to Q (h): Is service a paraprofessional service to individual? If “No” 33 42 If "Yes” Q (h): Is service a paraprofessional service to person age 21 or older? Proceed to If “No” 34 38 If "Yes” Per Review Guidelines, assure skills identified, beyond statement of activity, are clinical interventions, provided in order to empower the individual to learn the skills, and toward teaching/assisting the individual to become independent in the skill. 35 Enter “N” at “h.” Training in service definition required. Possible Internal Administrative Response. Q (h): Are measurable interventions related to skill building present? 36 If “No” If "Yes”
Enter “N” at “h.” Training in service definition required. Possible Internal Administrative Response. Q (h): Does goal reflect 1-on-1 intervention In community per service definition and Review Instructions? If "Yes” If “No” 37 Enter “Y” at “h.” Q (h): Is service a paraprofessional service to person under age 21? Proceed to If “No” 38 35 If "Yes” Proceed to If “No” Q (h): Is service provided in a school setting? 39 41 If "Yes” Per Review Guidelines, assure that interventions identified are clinically justified and are provided in order to assist the child in developing skills to function successfully and independently in the environment. 40 Enter “N” at “h.” Training in service definition required. Possible Internal Administrative Response. Q (h): Does goal reflect 1-on-1 intervention In community per service definition and Review Instructions? If "Yes” If “No” 41 Enter “Y” at “h.” Proceed to If “No” Q (h): Is service a Q-Level Service? 42 33 If "Yes”
Per Review Guidelines, assure that the note reflects Q-level activity such as coordination and oversight of initial and ongoing assessment activities, initial development and ongoing revision of the PCP or T/HP, monitoring of the implementation of the PCP or T/HP, and/or additional case management functions of linking, arranging for services and referrals. 43 Q (h): Does note reflect Appropriate QP activity per service definition and Review Instructions? Enter “N” at “h.” Training in service definition required. Possible Internal Administrative Response. If "Yes” If “No” 44 Enter “Y” at “h.” 45 Review Crisis Plan in PCP, or in T/HP. Q (i): Do the symptoms listed make sense with those indicated in assessments and treatment goals? Enter “N” at “i.” Training in service definition required. If “No” 46 If "Yes” Q (i): Do the strategies listed relate to the overall level and intensity of CS treatment provided? Enter “N” at “i.” Training in service definition required. If "Yes” If “No” Enter “Y” at “i.” 47 48 Review a sample of notes over the time period indicated. Recipient Not Appropriate. Refer to DMA. Possible Internal Administrative Response. Are service notes not individualized (canned, electronically copied)? 49 If “Yes”
Enter “N” at “j.” Training in service definition required. Q (j): Do the notes accurately relate to the diagnostic information previously reviewed? If "Yes” If “No” Enter “Y” at “j.” 50 Q (k): Do the notes accurately reflect the specific treatment goals in the PCP or T/HP? Enter “N” at “k.” Training in service definition required. If “No” If "Yes” Enter “Y” at “k.” 51 Enter “N” at “l.” Training in service definition required. Possible Internal Administrative Response. Q (l): Do the intensity (frequency and duration) of CS provided matches with services billed (paid claims)? If “No” If "Yes” Enter “Y” at “l.” 52 Review the service notes in the PCP or T/HP against the appropriate CS Service Definition (Child/Adult/Team). 53 Proceed to Q (m): Is service a direct service to individual? If “No” 54 56 If "Yes” Enter “N” at “m.” Training in service definition required. Possible Internal Administrative Response. Q (m): Does note reflect 1-on-1 intervention In community per service definition and Review Instructions? Enter “Y” at “m.” If "Yes” If “No” 55
Proceed to Q (m): Is service an indirect service to individual? If “No” 56 55 If "Yes” Enter “N” at “m.” Training in service definition required. Possible Internal Administrative Response. Q (m): Does note reflect Appropriate QP activity per service definition and Review Instructions? Enter “Y” at “m.” If "Yes” If “No” 57 Clinical Determinations (CD) based on Cumulative Information in Considerations (a) – (m) Enter “N” at “CD1.” Possible Internal Administrative Response. CD1: Is the CS service clinically necessary? If "Yes” If “No” Enter “Y” at “CD1.” 58 If “No” CD 1a: Would this individual be better served by access to more intensive services than CS? Proceed to If “No” 59 61 If "Yes” Identify suggested alternative services. 60
CD 2: Is the duration and frequency of the CS clinically appropriate? If "Yes” Enter “Y” at “CD2.” 61 If “No” Identify recommended duration and frequency. Possible Internal Administrative Response. 62 ADMINISTRATIVE (LME) RESPONSE ALTERNATIVES A1: Do the PCP or T/HP and treatment choices need additional review by LME staff to determine appropriateness? If “No” If "Yes” Enter “NA” at “A1.” Enter “Y” at “A1.” 63 Enter “Y” at “A2.” Possible Internal Administrative Response. A2: Is training in regard to the use of CS services needed? If "Yes” If “No” Enter “NA” at “A2.” 64 A3: Are the issues uncovered during this review beyond the scope of further review or training but warrant a Medicaid paid claims audit? Enter “Y” at “A3.” If "Yes” If “No” Enter “NA” at “A3.” 65
A4: Are the issues uncovered During this review beyond the scope of further review, training and/or a Medicaid paid claims audit, and referral to DMA for further review and investigation is warranted? If “No” Enter “NA” at “A3.” Enter “Y” at “A3.” If "Yes” 66