Febrile Neutropenia
Febrile Neutropenia. Mervat Hesham 2009. Febrile Neutropenia. Who should receive empirical Rx? When should empirical Rx be started? What is appropriate initial Rx? How should initial Rx be modified? How long should empirical Rx be continued?. Febrile neutropenia. *Fever


Febrile Neutropenia
E N D
Presentation Transcript
Febrile Neutropenia Mervat Hesham 2009
Febrile Neutropenia • Who should receive empirical Rx? • When should empirical Rx be started? • What is appropriate initial Rx? • How should initial Rx be modified? • How long should empirical Rx be continued?
Febrile neutropenia *Fever Single oral temperature > 38.3ºC OR • 38º C for more than 1 hour *Neutropenia • Neutrophils< 0.5x109/L (500/mm3) OR • Neutrophils <1.0 x109/L, predicted fall to < 0.5 x 109/L • Tympanic temperature (oral temperatures may be falsely high in presence of mucositis)
Neutropenia:(ANC) mild 1.0 to 1.5 x 103/l moderate 0.5 to 1.0 x 103/l Severe <0.5 x 103/l
Possible sites of infection • URTI • Dental sepsis • Mouth ulcers • Skin sores • Exit site of central venous catheters • Anal fissures • GIT • marrow aspiration sites • nails and nail peds, scalp
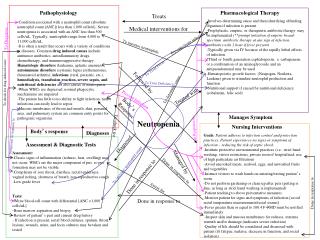
Factors Associated with Increased Risk of Infection • Duration and severity of neutropenia • type and intensity of chemotherapy • altered phagocytic, cellular and humoral immunity • breaches of skin and mucosal barrier • catheter or other foreign bodies • underlying diseases or therapy • corticosteroids
Pathogens • 60% - 70% of fevers during neutropenia have no identifiable etiology i.e fever of unknown origin. • Bacteremia seen in 10%- 20% of patients with fever and neutrpenia, Gram positive bacteremia 70% Gram negative bacteremia 30%
Common pathogen in neutropenia Bacteria: Gram positive organisms • Staphylococcus aureus • Coagulase-negative staphylococcus • alpha and beta hemolytic streptococcus Gram negative organisms • Escherichia coli • Klebsiella pneumoniae • Pseudomonas aeruginosa Fungi: • Candida , Aspergillus
Febrile Neutropenia Evaluation: • A. General measures: Attempt to reduce acquisition of resistant hospital pathogens in neutropenic patients by using the following precautions: • 1. Single-bed room (“protective isolation”). • 2. Wash hands with antibacterial soap prior to all patient contact. • 3. No live plants. • 4. Limit visitors. • 5. Meticulous skin care, especially IV catheter sites. • 6. Foley catheters, rectal thermometers, and suppositories should be avoided.
B. Avoid routine use of antipyretics and corticosteroids so that temperature trends and response to antibiotics can be monitored. Acetaminophen may be used for discomfort associated with fever. • C. Examine the patient frequently History : (cycle/course of chemotherapy,prophylactic agents, corticosteroids , immunosuppresive agents,previous infections or procedures).
Physical examination : *Signs(perianal erythema and tenderness, Minimal erythema or serous discharge at the site of a Hickman catheter, Signs & Symptoms of Sepsis (any one or more of the following signs): 1. Hyperpyrexia (Temperature > 104oF). 2. Hypothermia (< 96oF). 3. Chills not associated with transfusions or drugs 4. Hypotension (BP change > 30% or SPB < 90 mmHg; refer to age specific guidelines for children).
5. Hypoxemia (O2 saturation < 90% or > 5% change from baseline). 6. Moderate/severe End Organ Dysfunction (increased Scr or LFTs). 7. Altered Mental Status.
D . Risk assessment: • Low risk: • ANC > 100 /mm3 , • Normal CXR , • Duration of neutropenia< 7 d, • Resolution of neutropenia <10 d, • No appearance of illness, • No comorbidity complications , • Malignancy in remission. • High risk : • ANC < 100 /mm3 , • Duration of neutropenia > 7 d .
ُُE . Investigation • Full Blood Count -White cells, haemoglobin, platelets • Biochemistry -Electrolytes, urea, creatinine, Liver function • Microbiology -Blood cultures (peripheral and all central line lumens) -Exit site swabs -Wound swabs -Urine analysis and culture. -Stool analysis and culture. -+/- Cerebrospinal fluid • Radiology Baseline chest X-ray and any other X-ray indicated by exam. -+/- CT abdo/pelvis
F. Re-evaluate the patient daily (or more often if clinically indicated) for localizing signs of infection and for response to therapy. Unless the patient’s clinical status changes, allow at least 48 hours prior to modifying antibiotics. • G. Be alert for reappearance of fever in a patient who initially defervesces. This may indicate superinfection with resistant bacteria or with fungi.
Empirical Antibacterial Therapy Empiric antibiotic therapy Broad spectrum empiric antibiotic therapy must be started properly prior to organism identification. Survival is greater than 90% when patients are treated with appropriate empiric therapy.
Initial Empiric AntibioticsRationale • Severe risk of bacterial sepsis • Insensitivity of diagnostic tests • Delays in identification of pathogens
Febrile Neutropenia • Who should receive empirical Rx? • When should empirical Rx be started? • What is appropriate initial Rx? • How should initial Rx be modified? • How long should empirical Rx be continued?
Initial Empiric AntibioticsConsiderations • Broad spectrum of bactericidal activity • Local prevalence, susceptibility pattern • Antibiotic toxicity : well-tolerated, allergy • Host factors : severity of presentation • Prior antibiotic usage • Antibiotic costs • Ease of administration
Initial Empiric AntibioticsRecommended choices • Monotherapy • Duotherapy without vancomycin • Vancomycin plus one or two drugs
Oral Antibiotics and Outpatient Management • Current studies : potentially be safe and effective in low-risk patients
Monotherapy Choices • Ceph 3 : ceftazidime • Ceph 4 : cefepime • Carbapenem : imipenem , meropenem IDSA guidelines-2002
Combination TherapyAdvantages • Increased bactericidal activity • Potential synergistic effects • Broader antibacterial spectrum • Limits emergence of resistance
Combination TherapyDisadvantages • Drug toxicities • Drug interactions • Potential cost increase • Administration time
Combination TherapyChoices • Aminoglycoside + Anti-pseudomonal carboxypenicillin • Aminoglycoside + Anti-pseudomonal cephalosporin • Aminoglycoside + Carbapenem
Vancomycin as Empiric RxWhen to use ? • Known colonization with MRSA or PRSP • Clinically suspected serious catheter-related infections (eg bacteremia) • Hypotension or cardiovascular impairment • Initial positive results of blood culture for G+ bacteria
Febrile Neutropenia • Who should receive empirical Rx? • When should empirical Rx be started? • What is appropriate initial Rx? • How should initial Rx be modified? • How long should empirical Rx be continued?
Initial Antibiotic ModificationsConsiderations • Persistence of fever • Clinical deterioration • Culture results • Drug intolerance/side effects
Persistent FeverCauses • Nonbacterial infection • Resistant bacteria • Slow response to antibiotics • Fungal sepsis • Inadequate serum & tissue levels • Drug fever
Persistent Fever > 5 DaysChoices of Mx • Continue initial Rx • Change or add antibiotics • Add an antifungal drug(Ampho B)
Febrile Neutropenia • Who should receive empirical Rx? • When should empirical Rx be started? • What is appropriate initial Rx? • How should initial Rx be modified? • How long should empirical Rx be continued?
Duration of Antibiotic TherapyWhen to stop? • No infection identified after 3 days of Rx • ANC > 500 for 2 consecutive days • Afebrile > 48 hr • Clinically well
Empiricanti-fungal therapy • Give Antifungal therapy if • Prolonged neutropenic fever (>4 days) and on Broad spectrum antibiotics * Esophagitis , localized pulmonary infiltrate. * Failure of treatment of diffuse pulmonary infiltrate by I.V TMP and erythromycin . * Sinus tenderness or nasal ulcerative lesion. • Rationale • Fungal infections difficult to diagnose • High mortality, excess morbidity with delays in treatment • Advantages • Fewer fungal deaths • Disadvantages • >50% of patients will be treated unnecessarily • Toxicity of antifungals and costs +++
Empirical antianaerobe therapy • In perianal tenderness . • severe oral mucositis and gingivitis, acute abdominal pain ( typhilitis , appendicitis. (
Supportive measures in febrile neutropenia Colony Stimulating factors (G-CSF, GM-CSF)
Colony Stimulating factors in febrile neutropenia • Theoretical benefits • Reduce duration neutropenia • Reduce severity neutropenia • Reduce hospital stay • Reduce duration antibiotic therapy • Reduce alterations in chemotherapy regimens (dosage and timing) • Reduce infection-related mortality • Improve the effective delivery chemotherapy
Guidelines for use of CSF in febrile neutropenia • Primary prophylaxis • In chemo regimens with >40% risk of FN, most cost effective • Consider in pre-existing neutropenia, poor performance status, advanced malignancy • Secondary prophylaxis • If previous profound neutropenia, subsequent dose reduction preferred rather than giving CSF support with maximum intensity chemotherapy
Guidelines for use of CSF in other clinical settings • AML induction • Reduced duration neutropenia • No associated decrease in nadir, no reduction hospital stay, antibiotic usage or mortality risk • Trials esp in elderly variable • Combined chemotherapy and radiotherapy (mediastinal) • Relative Contraindication: increased risk thrombocytopenia • Febrile neutropenia with complicated sepsis • Adjuvant CSF given, benefit not confirmed
Hematopoietic growth factors : (a) Patients already on growth factors should continue on therapy if febrile neutropenia develops. There is no rationale to increase the dose. (b) Patients not on a growth factor should not be started unless certain prognostic factors predictive of clinical deterioration are present, including signs/symptoms of sepsis, pneumonia, or fungal infection. (c) Do NOT give growth factors if the patient is receiving concurrent radiation therapy – a more prolonged neutropenia may result.
Febrile NeutropeniaConclusions • Significant morbidity & mortality • Choice of initial empiric therapy dependent on epidemiologic & clinical factors • Monotherapy as efficacious as combination Rx • Modifications upon reassessment • Duration dependent on ANC
Antipseudomonal penicillin * I/V Piperacillin 200-300mg/kg/daily ( IV Divided q4–6h) *I/V Ticarcillin 300mg/kg/daily ( IV Divided q4–6h) • Aminoglycosides *I/V Gentamicin 6.0–7.5 mg/kg/daily. (Loaded with 2mg/kg IV Divided q8h) *I/V Amikacin 7.5mg/kg/12 hourly ( 15 mg/kg/day IV Divided q8h)
Monotherapy: • Monotherapy with certain broad spectrum antibiotic shown to be as effective as combination antibiotic regimen for empiric therapy. • Include, • Ceftazidime (3rd generation cephalosporin)( Fortum ) 100–150 mg/kg/day IV Divided q8h • Imipenam-cilastatin ( carbepenam ) I/V 12.5mg/kg/6 hourly Meropenem 0–120 mg/kg/day IV Divided q8h ( maximum dose 6 g/day) • Cefepime (4th generation cephalosporin) ( Maxipim) 50 mg/kg per dose IV Divided q8h or I/V 1-2gm/ 8 hourly
Oral antibiotic therapy: • Are acceptable for selective stable low risk patients. • Oral ciprofloxacin 750mg/8 hourly plus Amoxicillin/clavulanate500mg/8 hourly.