Download
1 / 54
1.21k likes | 3k Vues
Management of Febrile Neutropenia. Dr. Sameer Bakhshi Associate Professor Department of Medical Oncology Dr. B. R. A. Institute Rotary Cancer Hospital AIIMS, New Delhi. AIIMS is the largest hospital in India. There are 3.2 million patients seen in outpatient every year.

E N D
Management of Febrile Neutropenia Dr. SameerBakhshi Associate Professor Department of Medical Oncology Dr. B. R. A. Institute Rotary Cancer Hospital AIIMS, New Delhi
AIIMS is the largest hospital in India. • There are 3.2 million patients seen in outpatient every year.
IRCH has a load of 11000 new cancer cases/year and around 1000 of those are pediatric cancer cases. • It is one of the largest center for pediatric cancers in India.
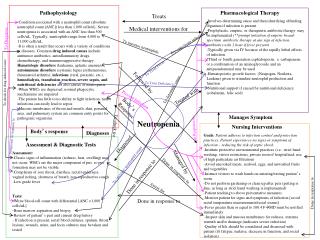
Why is a patient of Cancer Chemotherapy Immunocompromised? • Primary disease wherein normal BM is replaced with blasts leaving no normal cells. • Cytotoxic chemotherapy which results in • Granulocytopenia • Reduction in humoral and cell mediated immunity over prolonged administration • Presence of in-dwelling catheter, if any.
Neutropenia • Neutropenia is defined as Absolute Neutrophil Count (ANC) < 1500/mm³. • ANC = Neutrophil % x TLC • APC= [Neutrophil% + Monocyte %] x TLC
Febrile Neutropenia • Any fever > 101 F or 2 readings of 100.4 F 1 hour apart with ANC < 500/mm³. • Treat this as a MEDICAL EMERGENCY. • Risk of bacterial infection especially gram negative bacteria which if not treated early have >80% mortality. • May become a bigger reason for mortality than the actual malignancy.
Platelets WBC 0 5 10
Assessment of Neutropenia • Degree ANC 500-1500 ANC <500 ANC<100 • Phase Falling phase Nadir Rising phase. • Duration Is it prolonged neutropenia (> 5 days).
Assessment of Febrile Patient • Assess hemodynamic status • Skin and IV sites • Catheter • HEENT • Chest • Abdomen • Perianal area (Do not perform PR)
Investigations • Blood Culture from central line as well as periphery • Any other culture if required based on site of infection. • Chest X-ray
Therapy at Onset • Start intravenous antibiotics with a 3rd generation cephalosporin (Ceftazidime/ Cefepime) with an aminoglycoside. • Add gram positive coverage if any e/o: Catheter infection (staphylococcus) Severe mucositis (enterococcus) Pneumonia (high mortality).
A 14 year old boy with ALL in consolidation phase presented with personality changes. There was no fever and no FND. • MRI brain, biochemical parameters and CSF cell count and biochemistry was normal. • He was considered to have a psychiatric illness.
Acanthameba Meningitis Radhakrishnan, Bakhshi S PIDJ 2010
A 15-year-old boy with ALL on voriconazole prophylaxis developed nodular lesions in lung and thereafter developed maxillary swelling with septal perforation.
Nasal Mucormycosis Ganesan P, Bakhshi S JPHO 2009)
a b c d e f
Types of Febrile Neutropenia Low Risk FN High Risk FN Hematological cancers Duration of neutropenia > 7-10 days Increased risk of fungal infection • Solid tumors • Duration of neutropenia <7 days • Less risk of fungal infection
Treatment Plan • Patients were randomized to receive outpatient therapy with • Oral ofloxacin 7.5 mg/kg/dose every 12 hours and amoxycillin-clavulanate 12.5 mg/ kg (amoxycillin) every 8 hourly • Intravenous ceftriaxone 75 mg/kg/day and amikacin 15mg/kg once daily. • Prophylactic acyclovir and/or fluconazole if being used could be continued. • No growth factors were used.
A total of 123 episodes in 88 patients (67 males, 21 females) met the inclusion criteria and gave their consent for the study. • Sixty two of 123 episodes were randomized to the oral arm and 61 to the intravenous arm.
In the per protocol analysis treatment of febrile neutropenia was successful in 55 (93.2%) episodes in oral arm and 54 (93.10%) in intravenous arm. • Interestingly, therapy was equally successful in those who had ANC ≤ 100/L, ANC ≤ 200L, platelet counts ≤ 50,000/L and time to resolution of neutropenia ( ANC> 500L) more than 7 days in both the arms (p=NS)
Conclusions • This is the largest randomized study comparing oral and intravenous outpatient therapy upfront without concomitant use of growth factors. • Outpatient therapy is safe in pediatric LRFN with high success rates in both oral and intravenous therapy. • Thus, the combination of amoxicillin–clavulanate and ofloxacin may be used as an oral regimen of choice in pediatric LRFN.
Suggestions • In a hospital wishing to adopt this approach but hesitant to do so, it is important to maintain daily telephone contact with the patient. • Telephone contact helps in monitoring patient progress when patients are unable to come to the clinic daily, in times of emergency and also helps to ensure patient compliance. • The ability to provide emergency care when needed is important when patients are put on outpatient protocols.
High Risk Febrile Neutropenia • Acute Leukemia Induction • Consolidation Chemotherapy of Acute leukemias. What antibiotics to use?
Induction of Acute Leukemia • Assess and start chemotherapy. • We also initiate antifungal prophylaxis (AFP). • Majority patients are febrile at presentation.
Antifungal full doses are started earlier in case of development of pneumonia , hemodynamic instability even if before 5 days.
High Risk Febrile Neutropenia Outpatient Consolidation Chemotherapy in Pediatric Acute Myeloid Leukemia
Introduction and Rationale • Consolidation chemotherapy in AML results in prolonged neutropenia. Inpatient management is conventionally used in such intensive chemotherapy. • Problems with inpatient therapy: • High costs • Larger demand for existing inpatient resources • High risk of severe multi-resistant nosocomial infections • Demand/supply mismatch which may result in detrimental delays between chemotherapy cycles
44 cycles (63.8%) Managed entirely as outpatient 69 cycles (76.7%) Outpatient 25 cycles (36.2%) Needed admission Consolidation N=90 cycles 21 cycles (23.3%) Inpatient All managed in patient
Table 1A Abbreviations used: HIDAC-high dose cytosine arabinoside, CBC-complete blood count, LFT-liver function tests, RFT-renal function tests, PRP-platelet rich plasma, PRBC-packed red blood cells, FN-febrile neutropenia, GCSF-granulocyte colony stimulating factor, ANC-absolute neutrophil count.
Table IC: Abbreviations used: HIDAC-high dose cytosine arabinoside, CBC-complete blood count, LFT-liver function tests, RFT-renal function tests, PRP-platelet rich plasma, PRBC-packed red blood cells, FN-febrile neutropenia, GCSF-granulocyte colony stimulating factor, ANC-absolute neutrophil count.
Outcomes • The median number of blood draws for CBC, LFT and RFT were significantly lower in the outpatient group as compared to the inpatient group • Admission occurred during 25/69 (36.2%) of consolidation cycles planned as outpatient • All admissions were for febrile neutropenia but not all patients with febrile neutropenia met admission criteria
Length of hospital stay was significantly lower in the outpatient group • Saving of 269 patient-days for the entire study group. • There was one death during therapy in the outpatient consolidation group • Suspected intracranial bleed and sepsis • This patient was admitted for 2 days prior to death
Outpatient HIDACs leads to lesser number of blood draws but same number of transfusions and G-CSF use (similar supportive care) • Twice weekly blood draws were sufficient in the outpatient setting • Significant reduction of hospital stay in outpatient cycles
Similar incidence of Febrile neutropenia BUT in cycles administered as outpatient, there was significantly • Lesser duration of febrile neutropenia • Lesser use of second line antibiotics and antifungal agents • Lesser incidence of serious infections like pneumonia and/or septicemia
Conclusions • Outpatient AML consolidation therapy is safe and feasible in children • This service requires: • Dedicated day-care service • Daily telephonic contact with the patient and ability to offer emergency care when needed • In comparison with inpatient based therapy, it resulted in less frequent invasive blood draws; shorter duration of febrile neutropenia and consequently lesser antimicrobial and antifungal usage
Present Strategies • Low risk febrile neutropenia is managed outpatient. • More than 90% of AML consolidations are administered outpatient. • This has been possible because of a dedicated team effort.
Team/Services of Pediatric Oncology Services at AIIMS • Pediatric Oncologist • Pediatric Surgical Oncologist • Radiation oncologists with focussed interest in pediatric radiation oncology. • Radiologist/PET Scan/MIBG Therapy • Pathologists and Cytopathologist with focussed interest in pediatric malignancies. • Hematologists, laboratory oncologist. • Pediatric Stem Cell Transplant Facility