Download
1 / 57
570 likes | 615 Vues
Learn about clinical guidelines, diagnosis, symptoms, and treatment of endometriosis. Get insights from expert group recommendations. Enhance your clinical practice.

E N D
ESHRE GUIDELINE for the diagnosis and management ofendometriosis Thomas M. D’Hooghe, M.D., Ph.D. ESHRE SIG Endometriosis and Endometrium Leuven (Belgium) Postgraduate Course VWRG Leuven, 4th June 2010
LEARNING OBJECTIVES At the conclusion of this presentation, participants should be able to: 1. Summarize the development, updating and level of evidence associated with clinical guidelines in general 2. Apply the ESHRE guidelines for clinical management of endometriosis in their own clinical practice 3. Explain why many clinical issues with respect to endometriosis management are still unresolved and require more and better research.
Guideline Development Group Gerard Dunselmann Maastricht University (NL) Chair 2005-2007 Working party Andrew Prentice University of Cambridge (UK) Chair 2007-2010 Working party Charles Chapron Clinique Universitaire Baudelocque (F) Working party Robert Greb Münster University Hospital (D) Working party Thomas D’Hooghe Leuven University Hospital (B) Working party Daniela Hornung UFK Lübeck (G) Working party Lone Hummelshoj European Endometriosis Alliance (DK) Working party Stephen Kennedy University of Oxford (UK) Working party Ariel Revel University of Jerusalem (IS) Working party Ertan Saridogan University College London (UK) Working party http://guidelines.endometriosis.org
Recommendation: hierarchy of evidence http://guidelines.endometriosis.org
Recommendation:strength of evidence http://guidelines.endometriosis.org
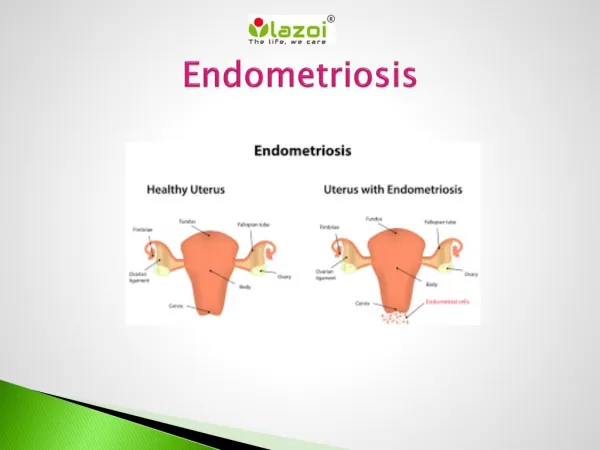
Localization and appearance • Pelvic organs and peritoneum • Minimal to severe (ASRM classification 1996, FS 1997) • Presentation: peritoneal, ovarian, deep • Peritoneal: typical/subtle (red, white, clear) • Ovarian endometriotic cyst/endometrioma • Deeply infiltrative endo (DIE): > 5 mm • Adhesions frozen pelvis http://guidelines.endometriosis.org
Symptoms • Variable presentation/often asymptomatic • Overlap with other conditions causing pain (IBS, PID, ..) • Delay between onset of symptoms and definitive diagnosis up to 12 years • Typical: severe dysmenorrhea, deep dyspareunia, CPP, cyclical pain associated with bowel or bladder http://guidelines.endometriosis.org
Clinical signs C http://guidelines.endometriosis.org
Diagnosis C http://guidelines.endometriosis.org
Diagnosis - histology GPP http://guidelines.endometriosis.org
Diagnosis - histology GPP GPP http://guidelines.endometriosis.org
Investigations: ultrasound A http://guidelines.endometriosis.org
At present, there is insufficient evidence to indicate that MRI is a useful test to diagnose or exclude endometriosis compared to laparoscopy. Investigations: MRI http://guidelines.endometriosis.org
Investigations: blood tests A http://guidelines.endometriosis.org
Investigations – disease extent GPP http://guidelines.endometriosis.org
Assessment of ovarian cysts GPP http://guidelines.endometriosis.org
Diagnosis - laparoscopy GPP GPP http://guidelines.endometriosis.org
Diagnosis - laparoscopy C C http://guidelines.endometriosis.org
PAIN – empirical w/o diagnosis GPP http://guidelines.endometriosis.org
PAIN (confirmed disease) -NSAIDs A It is important to note that NSAIDs have significant side effects, including gastric ulceration and an anti-ovulatory effect when taken mid-cycle. Other analgesics may be effective but there is insufficient evidence to make recommendations. http://guidelines.endometriosis.org
PAIN -hormonal Tx A There are pilot data suggesting that the aromatase inhibitor, letrozole, may be effective, though there are concerns about bone density loss (Ailawadi et al, 2004). http://guidelines.endometriosis.org
PAIN– duration of GnRH-a Tx A A http://guidelines.endometriosis.org
PAIN – hormonal Treatment The levonorgestrel intrauterine device (LNG IUS) may be effective in reducing endometriosis-associated pain (Vercellini et al, 1999) but there is insufficient evidence to make recommendations. Statement in publication 2005 - adapted in 2006 http://guidelines.endometriosis.org
PAIN – hormonal treatment A A systematic review identified two RCTs and three observational studies, all involving small numbers and a heterogeneous group of patients (Varma R et al, 2005). Nevertheless the evidence suggests that the LNG IUS reduces endometriosis-associated pain (Vercellini et al, 1999; Petta et al, 2005) with symptom control maintained over three years (Lockhat et al, 2005; Lockhat et al, 2004). Statement in revised guidelines 2006 http://guidelines.endometriosis.org
PAIN – HRT C http://guidelines.endometriosis.org
PAIN – surgical treatment A http://guidelines.endometriosis.org
PAIN – surgical treatment Pre-operative treatment A http://guidelines.endometriosis.org
PAIN – surgical treatment Post-operative treatment A http://guidelines.endometriosis.org
INFERTILITY – hormonal treatment A http://guidelines.endometriosis.org
INFERTILITY – surgical treatment A http://guidelines.endometriosis.org
INFERTILITY – surgical treatment B http://guidelines.endometriosis.org
INFERTILITY – surgical treatment A http://guidelines.endometriosis.org
INFERTILITY – surgical treatment Post-operative treatment A http://guidelines.endometriosis.org
INFERTILITY – ART: IUI A http://guidelines.endometriosis.org
INFERTILITY – ART: IVF B A The recommendation above is based on a systematic review but the working group noted that endometriosis does not adversely affect pregnancy rates in some large databases (e.g. SART and HFEA) http://guidelines.endometriosis.org
INFERTILITY – ART: COH for IVF B http://guidelines.endometriosis.org
INFERTILITY – ART: IVF and recurrence risk of endo B http://guidelines.endometriosis.org
INFERTILITY – ART: IVF A http://guidelines.endometriosis.org
INFERTILITY – ART: IVF A http://guidelines.endometriosis.org
INFERTILITY – ART: IVF GPP http://guidelines.endometriosis.org
EXTRAGENITAL ENDOMETRIOSIS B http://guidelines.endometriosis.org
Adolescents: Laparoscopic evaluation of chronic pelvic pain B http://guidelines.endometriosis.org
Adolescents: Laparoscopic Extent and appearance of endo B http://guidelines.endometriosis.org
Adolescents: Obstructive genital anomalies B http://guidelines.endometriosis.org
Coping with disease C http://guidelines.endometriosis.org
Coping with disease GPP GPP http://guidelines.endometriosis.org