Download
1 / 83
840 likes | 992 Vues
Pre-Hospital Obstetrics. Domenic Martinello, MD Assistant Director of Emergency Medicine EMS Medical Director Anna- Jaques Hospital Newburyport, MA. Objectives. I teach something You learn something Discuss general management of pregnant patients

E N D
Pre-Hospital Obstetrics Domenic Martinello, MD Assistant Director of Emergency Medicine EMS Medical Director Anna-Jaques Hospital Newburyport, MA
Objectives • I teach something • You learn something • Discuss general management of pregnant patients • Become familiar with standard techniques for delivery of a neonate • Review common problems during labour and how to manage them • Practice delivery using training aides
Outline • General Obstetrics • Third trimester bleeding • Abruptio placentae, placentae previa • Normal labour • Management and delivery • Post delivery care of mother and newborn • Labour issues • Shoulder Distocia • Breech Presentation • Cord Prolapse and Nuchal Cord • Preterm Labour • Post Delivery Problems • Uterine Rupture • Amniotic Fluid Embolus
Some quick notes • We will not be covering • Some Pregnancy emergencies BEFORE 20 weeks • Things like first trimester bleeding, ectopic, etc • Premature/Preterm rupture of membranes • Eclampsia and Preeclampsia • Gynecology • Management of pregnant patients during medical emergencies or trauma • They are all lectures unto themselves… • I can always come back for those!
Some general concepts • Normal pregnancy is 40 weeks • “term” pregnancy is any pregnancy that completes 37 weeks of gestation • Trimesters are essentially 14 week blocks • For you mathematicians you will realize this makes 42 total weeks. It is still correct because a portion of women will carry into 42 weeks. Some longer!
G’s and P’s • When talking about pregnant patients use the Gravida and Para scale • Gravida is number of pregnancies, regardless of outcome (including current!) • Parity is number of births >20 weeks (including stillborn) • Broken down into term, preterm, abortions (spontaneous or elective), and living children; note that multiples count as “1” for parity, but in the living children part it will count as 2. • Yes, this makes the number incredibly awkward • Thus, a patient who is currently pregnant and G7p5(4115) • Seven pregnancies • 5 deliveries >20 weeks, 4 term • one preterm • One abortion (miscarriage or elective) • 5 living children • Math: 4 term +1 preterm +1 abortion +currently pregnant = 7 • Easy, right?
Evaluation of the Pregnant Patient • As always, begin with the ABCs • Consider ALL female patients of childbearing age to be pregnant until confirmed otherwise! • You’d be surprised, but there are always some who go to term and never know it • I think there is a reality TV show to this nature • Determine due date and “how pregnant” patient is • Next slide will show some fun math
Wicked fun math • If the patient does not know her dates, ask for last menstrual period • More Math: Use Nagle’s rule to calculate EDC • EDC = Estimated Date of Confinement • Yes it is an odd term but it relates to the period of time a woman would classically be “confined” to bed rest to prevent pre-term labour • Nagle’s Rule: • Take date of LMP and add ONE YEAR • Then subtract 3 months • Then add 7 days • Example: If patient LMP is 8th of May 2009 • Make it 8th of may 2010; subtract 3 months to 8th of February 2010 • Then add 7 days to make it 15th of February 2009 for EDC!
Why do dates matter prehospital? • We need to know when you get to the ER • You need to know what you’re getting into if there is active labour • Foetal viability • This is controversial, so I’ll just give you some data since MANY providers use different thresholds based on their experiences and training • At 23 weeks of gestation there is 20%-35% survival • Between 24 and 25 weeks there is 50-70% survival • Between 26 and 27 weeks, survival is >90% • Note: weight threshold is 500g. It is essentially unheard of that a delivery under 500g will survive
Exam • Check for fundal height • 20 is just under umbilicus and 24 is just over • Rule of thumb: over umbilicus = viable • Heart tones heard 16-19 weeks • Rate: 120-160 BPM • Height does not apply with multiple Pregnancy conditions such as twins
Exam (2) • Quickening • Quick = alive (in Ye Olde English) • Quickening = foetal movement perceived by mother • Normally 18-20 weeks first felt • Multiparous women feel earlier, 15-17 weeks • May not be discernible by palpation until later • But you can ask mom!
Third Trimester Bleeding Abruptio, Previa, and other fun-to-say-but-really-bad-things
Third Trimester Bleeding • Major causes of bleeding are: • Abruptio placentae • Placentae previa • Premature labour • Lesions and lacerations of the genital tract
If you remember nothing else of this part… • NEVER NEVERNEVER conduct any form of digital examination on a bleeding pregnant patient in the second half of pregnancy • i.e. “nothing in a bleeding pregnant vagina after 20 weeks” • And I mean it… nothing. Don’t even consider it. Not even a peek. • Just leave it alone. • Seriously.
Abruptio Placentae • This is a cause of bleeding in which a normally implanted plancentae separates from the uterine wall • Occurs in 1% of pregnancies • May not be clinically significant • Is more frequent with any trauma! • HIGHLY associated with hypertension • Typically causes nausea, vomiting, back pain, abdominal pain, and usually (not always) vaginal bleeding • Pro-Tip: ANY painful bleeding in pregnant female near term is abruptio placentae until proven otherwise!
Abruptio continued • Maternal complications • Haemorrhagic shock • Hypotension • DIC (a complex coagulation dysfunction that consists of clotting and bleeding. Its “wicked bad”) • Uterine rupture • MOFS (multiple organ failure syndrome) • Sometimes called MODS (multi-organ dysfunction syndrome) • Foetal problems • Loss of blood flow leading to either severe neurologic injury or foetal loss and stillbirth
Abruptio pic • As with everything else, there are classifications.
Placentae Previa • This is a condition where the placentae implants partially or completely over the cervical os. • It also does cover a placentae that is “near” the cervical os, as it will usually be problematic during delivery • Causes PAINLESS vaginal bleeding near-term or at onset of delivery • Is notably different than any blood tinged mucous that is present during a normal delivery
In case you forgot • DO NOT DO ANY FORM OF INTERNAL EXAMINATION IN A PREGNANT PATIENT IN THE SECOND HALF OF PREGNANCY THAT HAS VAGINAL BLEEDING • This condition (placentae previa) is the reason… • If you do the examination and interact with the placenta that may be sitting inside an open or opening cervical os you can cause catastrophic haemorrhage and death • If you are uncertain… haemorrhagic shock and death is bad.
And once again… • These have various classifications:
So… why do we care? • Well, honestly, there is not much you can do prehospital for these • Much like there is little we can do in the ER with these • Both of these conditions require immediate OBGYN evaluation as they need C-Section deliveries sooner than later • But it is important to remember never to “go in” when there is bleeding in the second half of pregnancy and it is important to relay the information to the receiving hospital as many places will scramble an OR crew to be ready • In these cases, time is a precious commodity that is in short supply
Prehospitaltx for term-pregnancy with vaginal bleeding • “diesel injection” • “wheels down, shiny side up, and drive it like you stole it” • However you say it, get to a hospital with OBGYN capability!
Lets talk about the fun stuff now! Normal Labour and Delivery
Normal Labour and Delivery • The good news: • Precipitous delivery is relatively uncommon in modern medicine. • Success is encouraged by having preplanned kits for delivery and neonatal management • FREQUENT reassessment is absolutely necessary during transport
Questions to ask • Delivery date (EDC) and/or estimated dates • Presence of fluid (amniotic fluid) • Vaginal bleeding • Fetal movement • Delivery history • Prior problems with labour and delivery • Prior C-sections • Always get a medical and surgical history outside of the OBGYN issues
Assessment of maternal and foetal status • It is imperative when possible to assess fetal heart tones • It is worth the time spent if you can • Sometimes it is technically impossible • Doppler works best when available • Normal heart rate of the foetus is 120-160 BPM • Although a fast rate is bad, too slow of a rate is substantially worse
Membrane rupture • Premature Preterm Rupture of Membranes (PPROM) • Rupture without onset of labour AND before 37 weeks • Premature Rupture of Membranes • Rupture of membranes without onset of labour, after 37 weeks • Distinguishing the difference prehospitally is not terribly important. • It just happens that these are common causes of EMS transport
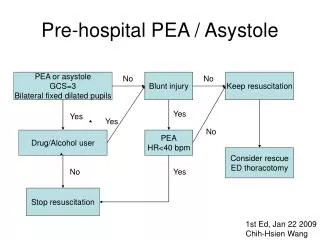
Stages of Labour • Different than stages of delivery • 4 Phases • Stage 1: Dilation • Stage 2: Foetal Expulsion • Stage 3: Plancental delivery • Stage 4: Post delivery phase • Sometimes used for the hours after Stage 3 completes • Also used to describe weeks afterward
Stages (pictorial) • Here is visual interpretation:
Stages of Delivery • Six phases: • Engagement of the foetalhead in the transverse position. The baby's head is facing across the pelvis at one or other of the mother's hips. • Descent and flexion of the foetalhead. • Internal rotation. The foetalhead rotates 90 degrees to the occipito-anteriour-position so that the baby's face is towards the mother's rectum. • Delivery by extension. The foetalhead passes out of the birth canal. Its head is tilted forwards so that the crown of its head leads the way through the vagina. • Restitution. The fetal head turns through 45 degrees to restore its normal relationship with the shoulders, which are still at an angle. • External rotation. The shoulders repeat the corkscrew movements of the head, which can be seen in the final movements of the foetalhead.
Your Role • Delivery of the head • Drape and prepare for delivery when the fetal station is low. • Meaning “crowning” or just before • Drapes and gowns protect the clinician from the fluid of delivery; sterile preparation is not required. • Its messy, so protect yourself; try and be as clean as possible • Use one hand to support and maintain the head in the flexed position as it delivers. • Use the other hand to support the perineum
Delivery of the head • Pics are great: • Note lower hand on perineum, upper holding the head
Delivery of the head (cont) • Control the pace of the delivery of the head. Maternal pushing is often helpful, but forceful pushing can cause the head to deliver too precipitously. • Have the mother momentarily withhold pushing once the head is delivered to check for nuchal cords. • Reduce nuchal cords (if present) if the mother and newborn are sufficiently stable to permit a pause in delivery.
Delivery of the Shoulders • Head is out, shoulders are next! • With both hands on the head, support delivery of the shoulders one at a time as the mother pushes with a contraction. • Without pulling, apply gentle posteriourtraction of the head at an angle of 45° to deliver the anteriourshoulder followed by gentle anteriourtraction of the head to deliver the posteriour shoulder • ProTip: DO NOT pull the head off the baby. Its bad form and is really hard to fix
Anteriour Shoulder • First
And… the posteriour • Remember: don’t pull on the head • Hard to fix. Seriously.
Delivery of the Body • Under normal circumstances this happens fairly easily • All you need to do is control the newborn, support the head, and GENTLY assist the baby out • Don’t pull on the head • I probably did not mention this yet. But, don’t. • I’m serious. • Really serious • It causes “badness” • Hard to fix. • Before stimulating the baby suction mouth and nose
Clamp the cord • New ProTip: It is NOT NOTNOT necessary to IMMEDIATELY cut the cord. • Actually, it has been shown a delay of greater than 30 seconds is beneficial to the newborn • No… I don’t know why. • How To: Place 2 umbilical clamps several centimeters apart and… well… cut between them!
Delivery complete? • No! • Dry, wrap, warm the infant. • Give infant to mom if stable and normal • APGAR score • Fun Fact: is an acronym designed by Dr. Virginia Apgar who was an anaesthesiologist • Was actually designed to be used during neonatal anaesthesia • Components: Appearance, Pulse, Grimmace, Activity, Respiration • Other acronym: “How Ready Is This Child”, which summarizes the test criteria as Heart rate, Respiratory effort, Irritability, Tone, and Color • Each gets a score from 0-2
APGAR • 1 minute and 5 minutes
Delivery of the Placenta • Placental separation is evidenced by the following: • An increase in umbilical cord slack • A bolus of blood from the uterus • Superior migration of the uterus within the abdomen with an increase in uterine firmness • The clinician can facilitate placental delivery. • Apply gentle traction on the umbilical cord with one hand. • Apply vertical pressure just superior to the pubic symphysis with the other hand to prevent inversion of the uterus. • Administer intravenous oxytocin to expedite the third stage of labor. Oxytocin should be started at delivery of the anterior shoulder. • Inspect the placenta after delivery. • Manually explore the uterus if the placenta is not intact. • Retained placenta fragments increase the risk of postpartum hemorrhage.
You’ve done it! • People have been delivering babies since the dawn of time without any medical training. Just remember that. • If you are not sure what to do remember that all YOUR job mandates is determining there is not an emergency that should halt labour, transport, and assisting the mother through the process. • If ALL else fails and you panic, make sure you see a head, no cord, not too much blood, and let the delivery naturally happen while your partner drives the ambulance “wikkid fast”.
And the not-so-fun stuff Abnormal Labour Conditions and Difficult Delivery Shoulder dystocia, nuchal cord, cord prolapse, and breech delivery
Shoulder Dystocia • Impaction of the foetal shoulder agianst the maternal pelvic outlet • Happens after delivery of the head • USUALLY is the anteriour shoulder against the pubis • More common in large infants (macrosomia) • Also more common when there have been prior shoulder dystocias (importance of history!)
Why is it bad? • Can cause SIGNIFICANT morbidity and mortality ifnot noted and managed • Foetal brachial plexus injuries • Hypoxia from cord compression • Highly litigated problem
How do you notice dystocia of the shoulder? • After delivering the foetal head you typically need only a small amount of downward traction • If the head comes out it may retract tightly against the perineum, often called “turtle sign” • If this happens you have options: • Use the momentum from the head delivery to deliver the shoulder (it does work sometimes) • There are some more difficult techniques (next page)
Delivering the “stuck” shoulder • Step 1: GET HELP • Get assistance and mark the TIME the shoulder dystocia started. This is important for the OBGYNs • Step 2: McRoberts Maneuver • “extreme lithotomy” position • Legs sharply flexed to the abdomen • Held by mother and/or assistant
Delivering “stuck” shoulder (2) • Step 3: • If possible drain bladder • If allowed a GENEROUS episiotomy • Ewww… • No, I will not suture it all back together for you, you break it you buy it • Step 4 • Assistant should apply suprapubic pressure • This may help dislodge the stuck shoulder • DO NOT apply fundal pressure, it will lock the shoulder harder against the pelvis
Stuck Shoulder (3) • Step 5 • If those maneuvers do not work, you are “screwed” • Well, you have to use the Woods Corkscrew Maneuver • Place 2-fingers behind the posteriour shoulder of the foetusand grasp the scapula • Rotate the infant 180 degrees • Rotates the anteriour shoulder posteriourly and the posteriour shoulder anteriourly • Have mother push and deliver “obliquely” through the pelvis
Stuck Shoulder – Last ditch! • Step 6: • If STILL unsuccessful… DO NOT PANIC • Deliver the posteriour shoulder first • Place your hand posteriourly into the vagina • Grasp the elbow and flex the arm at the elbow • apply gentle traction to deliver the posteriour shoulder and arm • This will release the anteriour shoulder • Whatever works, then continue normal delivery







![OBSTETRICS [SURGICOSE]](https://cdn4.slideserve.com/8057050/medical-instruments-medical-instruments-dt.jpg)