Neonatal Herpes Simplex Infections
420 likes | 1.28k Vues
Neonatal Herpes Simplex Infections. MAJ Mark Burnett Pediatric ID Fellow MAR 2003. Neonatal Herpes. Background A Case Study Types of Infections Risks of Infection Diagnostics Treatment Summary. “Herpes” – from the Greek “to creep, crawl”

Neonatal Herpes Simplex Infections
E N D
Presentation Transcript
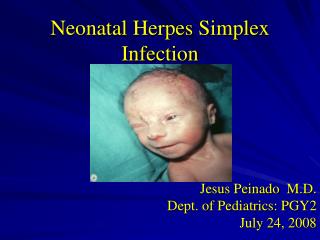
Neonatal Herpes Simplex Infections MAJ Mark Burnett Pediatric ID Fellow MAR 2003
Neonatal Herpes • Background • A Case Study • Types of Infections • Risks of Infection • Diagnostics • Treatment • Summary
“Herpes” – from the Greek “to creep, crawl” “Herpetic eruptions” described as early as 100 AD 1960’s – HSV1 and HSV2 differentiated HHV1 – HSV1 HHV2 – HSV2 HHV3 – VZV HHV4 – EBV HHV5 – CMV HHV6 – Causes? HHV7 – HHV8 - Herpes Infections
A Case Study – A.B. • Term infant born to a 22 y/o GBS+ mother with no Pmhx of HSV-2 • 4 doses of IV PCN given PTD • ROM <18 hours PTD, no maternal fevers • Forceps delivery • APGARS of 9/9 • Well until fever to 101.7 at 30 hrs of life • Fever work-up initiated
A.B. • WBC 23K (50S 2B 38L) • AST 98 ALT 92 • CSF 48 WBC 2650 RBC Pro 93/Glu 53 • HSV PCR, Enteroviral PCR, HSV Surface cx – sent • Exam unremarkable • Amp/Gent/Acyclovir initiated • Fevers persisted over next 13 hours, again spiking to 101.5 • AST 147 / ALT 93 two days later
A.B. – additional info • No history of HSV reported in mother, father • Mother without febrile illness • Niece with a “cold sore” visited prior to delivery, and “held the baby” after he was born • LP repeated two days after initial study with normalization of cell count
Questions? • What diagnostic tests could we perform, and how reliable are they really? • Would it be worthwhile to run tests on mom? • Is the niece’s “cold sore” a “red herring” – what are the risks? • Bottom line – how worried should we be about HSV, and how would we treat it?
Neonatal HSV • 1 in 2,500-5,000 deliveries / 500-1500 per yr. • Birth to 7 weeks of life • HSV2 = 70-75%, HSV1 = 25-30% • 3 Main Types • Skin, Eye, Mouth (SEM) • CNS • Disseminated Disease (DISSEM) • At Risk: Premature, ROM >6hr, Fetal scalp monitoring • Can be acquired congenitally, during the birth process, and in the post-partum period
Routes of Transmission • 85% via infected maternal genital tract • Ascending infection? • En route • 10% postpartum • 5% (or less) – intrauterine/congenital infection
Congenital HSV • Rare, most devastating • Only 50 cases described • Skin vesicles • Chorioretinitis • Microcephaly • Micro-ophthalmia • IUGR
Skin, Eye, Mouth (SEM) • Approximately ½ of all HSV infections • 1st-2nd week presentation • Limited to skin, eye, mouth/mucous membranes • 60-70% of untreated patients progress to CNS/disseminated disease
SEM (cont) • Long term neurologic sequelae seen in 30% of cases – even if treated • Ophthalmology involvement
HSV - CNS Disease • Encephalitis without visceral involvement, mainly involving the temporal lobes • Early to 3rd week of life presentation • Skin lesions may appear late, if at all • 35% of all cases, only 2-5% untreated survive normally
Disseminated Disease • Approximately 20% of all infections • Hepatitis • Pneumonitis • DIC • Infant may be ill on first day of life • Skin lesions appear late, or not at all
Postnatal acquisition • Most commonly HSV1 • Moms with HSV • Mask • Breastfeeding – O.K. if without lesions • The Mohel and the Mezizah
Contacts • “Personnel with an active herpetic whitlow should not have direct patient care of neonates”. • Family transmission has been described
Take Home Message • Infection is most common when a mother develops a genital infection late in pregnancy ( her primary HSV1 or HSV2 infection) – then delivers before the development of protective maternal antibodies
Herpes Simplex • Approximately 5% of the general population has been diagnosed with genital herpes – but approximately 20-30% of women may be infected with HSV-2 • Viral shedding occurs without identifiable lesions on 1-3% of days
Maternal Testing? • Identify discordant couples to avoid transmission in the third trimester • If mom is HSV1/HSV2 negative • If mom is HSV2 negative • If mom is HSV2 positive – risk is low for a vaginal delivery? • Is testing after delivery going to be helpful? • Will blood tests of the baby be helpful, or just reflect mom’s status? • Psychosocial ramifications?
Herpes during Pregnancy • As many as 2% of pregnant women are infected with HSV2 during pregnancy • 25% of women with a history of genital herpes have an outbreak at some time during their pregnancy, 11-14% at time of delivery • 36% at delivery for those with first infection! • Virus is recovered from 1% of asymptomatic women at delivery
What is the risk? • Vaginal delivery when mom has presence of first symptomatic lesions – 50% • Vaginal delivery when mom is asymptomatic, but is newly infected – 33% • Vaginal delivery when mom has recurrent lesions – 4% • Vaginal delivery when mom has a history of herpes lesions in past, none presently – 0.04%
OB Management • 70’s-80’s – weekly HSV cultures • 1988 – patient examined at delivery, Cesarean delivery if: (no data) • Identifiable genital lesions • Patient describes prodromal symptoms • Vaginal delivery for those with hx only • Primary infection diagnosed - treat • Estimated $2-4 million to prevent each case • 20-30% of infants who are diagnosed with neonatal herpes are delivered by Cesarean delivery
Diagnostics • HSV Cx – positive in 1-2 days (cytopathic effect) • DFA – sensitivity/specificity in the 75%-85% range
PCR Testing • Detects minute amounts of DNA, RNA • DISSEM – 93% • CNS – 76% • SEM – 24% • False negative may occur if CSF is obtained “too early” • Order through IVF!
Diagnostics (cont) • Surface cultures • Mouth (40-50%) • Eyes (25%) • Rectum • Skin • Cultures • Stool • Urine • CSF >100 WBC/Inc. Pro • Tzanck – neither sensitive nor specific
Treatment - Acyclovir • SEM infections • 60mg/kg/day divided q8h for 14 days • May be lengthened to 21 days in the near future • Oral Acyclovir needed later in life? • DISSEM and CNS HSV infections • 60mg/kg/day divided q8h for 21 days • Re-tap if CNS disease exists prior to d/c • Watch for neutropenia – 2x week ANCs
Questions / Controversies • Would maternal “pre-treatment” change the time /clinical presentation of HSV? • Should an infant delivered vaginally to a mother with active lesions be treated? • Can HSV be resistant to Acyclovir?
Take Home Messages • Most neonates with HSV infection are born to mothers with asymptomatic genital shedding at delivery, with no history of genital herpetic lesions • No one test is 100% sensitive / specific • Keep HSV in mind • How would you manage our case?