Personal Information Form for Healthcare
10 likes | 102 Vues
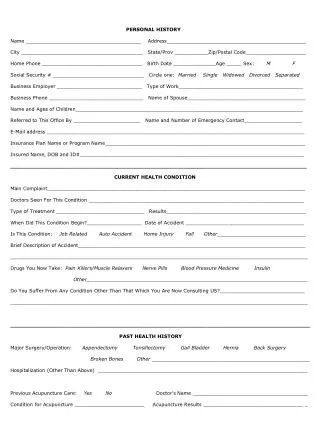
Complete this form with your personal and medical details before consultation. Include contact info, health condition, past history, and insurance coverage.

Personal Information Form for Healthcare
E N D
Presentation Transcript
PERSONAL HISTORY Name ______________________________________ Address______________________________________________ City ________________________________________ State/Prov ___________Zip/Postal Code____________________ Home Phone _________________________________ Birth Date ______________Age _____ Sex: M F Social Security # ______________________________ Circle one: Married Single Widowed Divorced Separated Business Employer ____________________________ Type of Work_________________________________________ Business Phone _______________________________ Name of Spouse_______________________________________ Name and Ages of Children___________________________________________________________________________ Referred to This Office By ______________________ Name and Number of Emergency Contact___________________ E-Mail address _____________________________________________________________________________________ Insurance Plan Name or Program Name__________________________________________________________________ Insured Name, DOB and ID#__________________________________________________________________________ _______________________________________________________________________________________ CURRENT HEALTH CONDITION Main Complaint_____________________________________________________________________________________ Doctors Seen For This Condition _______________________________________________________________________ Type of Treatment _____________________________ Results______________________________________________ When Did This Condition Begin?__________________ Date of Accident _______________________________________ Is This Condition: Job Related Auto Accident Home Injury Fall Other_____________________________ Brief Description of Accident___________________________________________________________________________ __________________________________________________________________________________________________ Drugs You Now Take: Pain Killers/Muscle Relaxers Nerve Pills Blood Pressure Medicine Insulin Other_________________________________________________________________________ Do You Suffer From Any Condition Other Than That Which You Are Now Consulting US?____________________________ __________________________________________________________________________________________________ ________________________________________________________________________________________ PAST HEALTH HISTORY Major Surgery/Operation: Appendectomy Tonsillectomy Gall Bladder Hernia Back Surgery Broken Bones Other ____________________________________________________ Hospitalization (Other Than Above) _____________________________________________________________________ Previous Acupuncture Care: Yes No Doctor’s Name ______________________________________ Condition for Acupuncture _______________________ Acupuncture Results _________________________________ _