Download
1 / 36
560 likes | 1.01k Vues
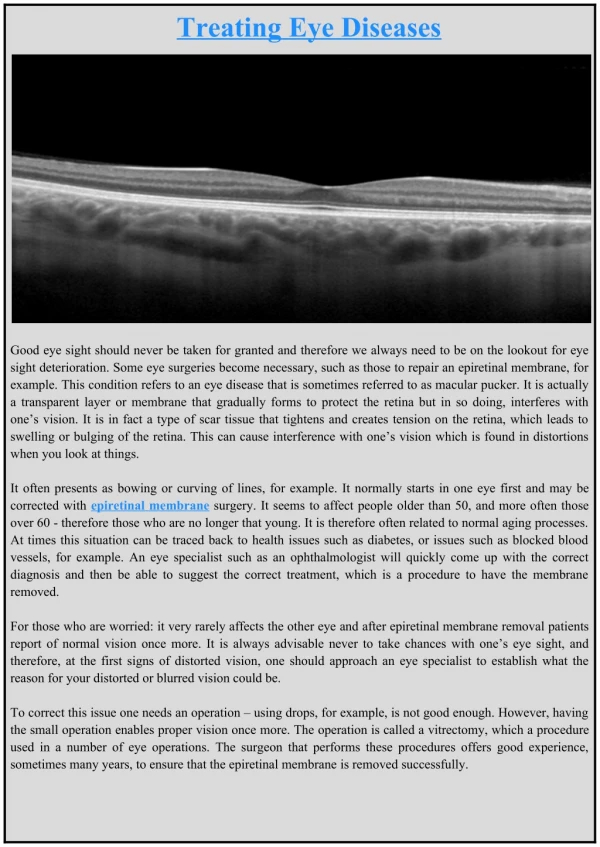
Eye In Systemic Diseases. Prepared By: Moath A. Nassar. Systemic Diseases ?. Systemic diseases are diseases that involve many organs or the whole body. Many of these diseases also affect the eyes . In fact, an eye exam sometimes leads to the first diagnosis of a systemic disease.

E N D
Eye In Systemic Diseases Prepared By: Moath A. Nassar
Systemic Diseases ? • Systemic diseases are diseases that involve many organs or the whole body. • Many of these diseases also affect the eyes. • In fact, an eye exam sometimes leads to the first diagnosis of a systemic disease Why is the eye so important in systemic disease? The eye is composed of many different types of tissues. This unique feature makes the eye susceptible to a wide variety of diseases as well as provides insights into many body systems.
Systemic diseases to be discussed : • Collagen vascular disease • Spondyloarthropathies • Sarcoidosis • Systemic vasculitis • Blood disorders • Demyelinating disorders • Hypertention and vascular diseases • Thyroid disorders • General signs & symptoms • Diagnostic tests • General management • Ocular involvement • Signs & symptoms • Treatment and prognosis
1.Collagen vascular disease • problems with the immune system affect collagen • wide category of diseases • Symptoms of collagen vascular disease vary from disease to disease, but may include: • Back pain • Chest pain and shortness of breath • Fatigue and weakness • Fever • Painful, swollen joints • Rashes • Diagnosis • Hx & physical examination, Blood tests can check level of autoantibodies, • RF, urinalysis ,LFT , KFT , ESR, C- XR • Treatment • Some may go into remission spontaneously • Depends on the extent of the disease • Steroids or anti-inflammatory medications to ease discomfort • In advanced cases, immunosuppressant drugs may help
a. Behçet's disease • Recurrent multisystemic disease presented during third to fourh decade • Major diagnostic criteria : • Recurrent oral aphthousstomatitis • Skin lesions ( erythemanodosum,…) • Recurrent genital ulceration • Uveitis : both anterior and posterior • Minor diagnostic criteria • Arthritis , epididymitis, intestinal ulceration , neurological and vascular complications • Four major criteria simultaneously or at different times is diagnostic
Hypopyon which can be seen in anterior uveitis in a patient with Behcet's disease. • Acuteanterioruveitis generally responds to corticosteroid eye drops. • Inflammation involving the back of the eye requires treatment that is more aggressive with corticosteroids given by injection and/or pill (systemic therapy). • may lead to blindness in 20% of those affected
b. Sjögren'ssyndrome • Autoimmune inflammation and destruction of lacrimal and salivary glands • Primary or secondary • F>M • Presented in adult life with gritteness( sandiness) of eyes and dryness of the mouth • Signs • Large salivary glands with diminished salivary flow • Dry nasal passages • Raynaud’s phenomenon • Diagnosed by serum autoantibodies and biopsies • Ophthalmic features • Common :Keratoconjunctivitissicca • Rare : adie pupil • Treatment • If mild tear substitutes would help • Avoiding low humidity environment • Occluding the punctum in severe cases
keratoconjunctivitissicca Complete cure could never be achieved but fowolloing a strict treatment guidelines may improve the outcome
c. Systemic Lupus Erythematosus • Autoimmune non-organ specific connective tissue disease • F>M • Presented during third to fifth decade with fatiguabilty without specific organ involvement • Signs • Mucocutaneous, musculoskeletal, renal, cardiovascular, pulmonary, haemopoitic, reticuloendothelial, neurological. • Diagnosis: ESR is raised, C- ractive protein is normal, serology. • Treated by steriods and cytotoxic agents • Ophthalmic complications • Common: Madarosis and keratoconjunctivitissicca • Uncommon: peripheral ulcerative keratitis • Rare: scleritis, retinal vasculitis and optic neuropathy
Madarosis is the absence or loss of the eyelashes (and sometimes the eyebrows) Discoid lesions is the cause in this case
d. Rheumatoid arthritis • Autoimmune systemic disease characterized by symmetrical, destructive, deformating, inflammatory, polyarthropathy • F>m • Presented during the fourth decade and occasionally during the childhood • Signs • Arthritis ( symmetrical involvement of small joints of hands and feet, ulnar deviation ,…) • Skin ( raynaud’s phenomenon, vasculitis , …) • Treated by NSAIDs, cytotoxic drugs ,… • Ophthalmic features • Common: keratoconjunctivitissicca ( secondary ) • Uncommon: scleritis and peripheral ulcerative keratitis • Rare: acquired superior oblique tendon sheath syndrome
Scleromalacia ; potential perforation tumour necrosis factor (TNF) blockers (infliximab) are effective therapeutic agents in ocular complications of rheumatoid arthritis
e. Systemic scleroderma • Chronic connective tissue disease affecting the skin and internal organs • F>M • May be limited , diffuse and overlapping with other autoimmune diseases • Presented in the fourth to sixth decade with raynaud phenomenon • Signs: • Skin: tightening and thickening on hands , feet , face and trunk. Subcutaneous fibrosis, typical facial appearance( fixed expression, restrictive movements of lips and “ beaking of nose) • Organs: esophageal dysmotility, heart , lung and kidney disease, mild arthritis • Diagnosis: serology • Treatment: Immunosuppressive agents, Antifibrotic agents, Anti-infammatory agents,….. • Ophthalmic features • Common: eyelid tightening and telangectasia • Uncommon: keratoconjunctivitissicca
Skin tightening on the face ( including the eyelids) Telangiectasia
2.Spondyloarthropathies • Group of inflammatory joint diseases including: • Ankylosingspondylitis • Reactive arthritis( reiter’s syndrome ) • Psoriatic arthropathy • Arthritis associated with inflammatory bowel disease(enteropathicspondylitis ) • Isolated acute anterior uveitis • An association with HLA –B27 occurs in all of them but in particularly strong for ankylosingsponndylitis ( > 95%) and reiter’s disease ( 90 %) • They share common clinical features: • Asymmetrical inflammatory oligoarthritis, Sacroiliitis and inflammatory spondylitis • Diagnosis: Hx , exam ,radiographs, HLA B- 27, serology • Ophthalmic features: • Thay all cause acute anterior uveitis • conjunctivitis, keratitis, keratoconjunctivitissicca, scleritis
Recurrent Iritis caused Synechiae(adhesions between the lens and iris) in ankylosingspondylitis
Conjunctivitis (figure) is a common ophthalmic feature of Reiter's syndrome along with acute anterior uveitis • corneal infiltrate is Uncommon feature Conjunctivitis is not very painful, does not affect vision, and is not serious and goes without treatment
Scleritis in Crohn disease If mild, could be treated by NSAIDs but if severe , systemic steriods may be introduced Also we may have conjunctivitis , peripheral corneal infiltrate & retinal periphlebitis in Crohn disease
3.Sarcoidosis • Multi- systemic granulumatous inflammatory disorder • Presentaion: • Acute onset sarcoidosis typically occurs during the third decade • Insidious onset sarcoidosis occurs during the fifth decade • Signs • Pulmonary : in 90 % of patients, ranges from asymptomatic bilateral hilarlymphadenopathy to progressive pulmonary fibrosis and bronchectasis • Skin : erythemanodosum, granuloma • Neurological : cranial nerve palsies ( particularly facial) , intra cranial granuloma • Diagnosis: • Chest radiographs • Biopsy : • Lungs , gives the greatest yield • Conjunctiva , positive in about 70 % • Lacrimal glands, positve in 25 % of unenlarged and 75 % of enlarged • Calcium assay
Treatment options include NSAIDs steroids and low dose cytotoxic agents • Ophthalmic features • Common : conjunctivalgranulomas, anterior uveitis, posterior uveitis and retinal periphlebitis • Uncommon : keratoconjunctivitissicca and intermediate uveitis • Rare: fundusgranulomas, retinal and disc neovascularization, and papilloedema Mild symptoms are treated by topical steroids and cycloplegics. Systemic steroids are indicated in cases not responding to topical steroids
Anterior segment granulomatous involvement in a case of ocular sarcoidosis
A: Scattered peripheral multifocal lesions characteristic of ocular sarcoidosis. B: The macula of the same patient demonstrating a choroidalneovascular membrane.
4.Systemic vasculitis • The systemic vasculitides are characterized by inflammation of blood vessel walls • Vessels of any type, in any organ can be affected, • classified based on affected vessel size (large, medium, and small) • Signs and symptoms • Nonspecific complaints • Those should raise a strong suspicion: • Mononeuritis multiplex, palpaplepurpura, pulmonary renal syndrome • Diagniosis : a compatible clinical presentation supported by specific laboratory or imaging tests and confirmatory histology • Glucocorticoids are the primary treatment for many forms of vasculitis , Additional immunosuppressive agents are sometimes required
a. Giant cell arteritis • A granulumatous necrotizing arteritis with predilection for large and medium size arteries , particularly the superficial temporal , ophthalmic, posterior ciliary and proximal vertebral • Presented during the seventh to eighth decade with the following: • Scalp tenderness, headach, jaw claudication (pthognomonic) , polymyalgiarheumatica , non specifc symptoms, blindness ( sudden with minimal systemic upset), superficial temporal arteritis ( thick , tender, inlammed, and nodular arteries which can’t be flattened against the skull), the pulsation later ceases which strongly suggestive of GCA • Diagnostic tests • High ESR , CRP • Temporal artery biopsy should be performed • Treatment : by administration of systemic steriods
Ophthalmic features • Common: anterior ischemic optic neuropathy • Uncommon: cotton wool spots, central retinal artery occlusion , ocular motor nerve palsy ( commonly a pupil sparing third nerve palsy ) • Rare: ocular ischemic syndrome Typical findings of a patient with arteritic ischemic optic neuropathy. Note the pallid disk edema, associated hemorrhages, and adjacent cotton wool spot Treatment for arteritic ischemic optic neuropathy is CORTICOSTEROID MEDICATIONS
b. Polyarteritisnodosa • Idoipathic , potentially lethal , collagen vascular disease affecting medium sized and small arteries • Presented during the sixth decade • Signs • Skin: purpura and easy bruising , gangrene • Muscles: weakness and tenderness • Complications • Renal involvement and hypertension • Coronary arteritis • GI bleeding • Stroke or multifocal neuropathy • Diagnosis: skin biopsy • Treatment: systemic steriods and immunosuppressive agents
Ophthalmic features • Common: peripheral ulcerative keratitis and scleritis • Rare: orbital pseudo-tumour and occlusive retinal periarteritis Peripheral ulcerative keratitis presents with a crescent shaped destructive lesion of the juxtalimbal corneal stroma
c. Wegener’s granulomatosis • Idiopathic , multisystem, granulomatous disorder characterized by generalized small-vessel vasculitis affecting predominantly the respiratory tract and the kidneys • Presented in the fifth decade , often with pulmonary symptoms • Signs • Respiratory tract • Upper: perforation of the nasal septum • Lower: nodular lesions , infiltrates and cavitaions • Organs • Necrotizing glomerulonephritis with renal failure • Affects heart , spleen and adrenals • Neurological: polyneuritis and meningoencephalitis • Diagnosis: Anti-neutrophil cytoplasm antibodies • Treated with systemic steriods and cyclophosphamide
Ophthalmic features • Common : nasolacrimal obstruction and dacrycystitis • Uncommon: scleritis and peripheral ulcerative keratitis • Rare: orbital pseudo- tumour and occlusive retinal periarteritis Nasolacrimal duct involvement can result in epiphora, dacryocystitis and draining fistulas. sclerokeratitis Dacrocystitis treated by surgey (Dacryocystorhinostomy ) . Good outcome
5.Hematologic disorders • Hematological diseases encompass a wide spectrum of disorders ranging from benign to malignant conditions that can present with ocular involvement • Ocular findings related to anemia, hematological malignancies and platelet disorders are to be disscussed
a. Anemia • Anemia is a common condition that occurs when the level of healthy RBCs or Hb is below normal • Causes include: destruction, increased blood loss and inadequate production of RBCs by the bone marrow • Additional causes related to poor nutrition or absorption defects in the GI tract include iron, vitamin B12or folic acid deficiencies • general symptoms: pallor of the skin or nail beds, weakness, headaches, shortness of breath, GI disturbances, fever, and numbness or coldness of extremities • Diagnosis: CBC is the most important, assess level of B12 and folic acid, bone marrow biopsy
Ocular changes • conjunctival pallor and hemorrhages • anemic retinopathy(intraretinal hemorrhages, Roth’s spot hemorrhages, cotton-wool spots, retinal exudates, venous dilation and optic nerve pallor) • These changes generally occur in patients with severe anemia or when thrombocytopenia is present
Sickle cell anemia may also cause sickledconjunctival vessels, central retinal artery occlusion (CRAO), branch retinal artery occlusion (BRAO), sicklingmaculopathy
c. Platelets disorders • Ocular changes can include : • Conjunctivalpetechial hemorrhages • Amaurosisfugax • Vascular occlusions • Retinal, vitreal and choroidal hemorrhages