Download
1 / 36
380 likes | 888 Vues
Anemia in children of different age. Lecturer: Sakharova Inna.Ye., MD, PhD. Anemia is defined as hematocrit (Hct) , hemoglobin (Hb) , red blood cells (RBC) concentration >2 SD below mean for age. Prevalence of anemia in INDIA (WHO reports 2002-2003)

E N D
Anemia in children of different age. Lecturer: Sakharova Inna.Ye., MD, PhD.
Anemia is defined as hematocrit (Hct), hemoglobin (Hb), red blood cells (RBC) concentration >2 SD below mean for age.
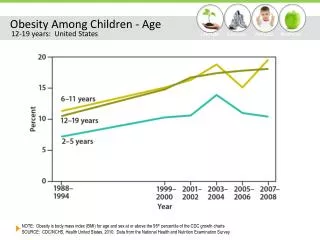
Prevalence of anemia in INDIA (WHO reports 2002-2003) • 7 states (Assam, HP, Hy, Kerala, MP, Orissa, TN )– 86.1%of pregnant womenhaveanemia (Hb <70g/L-9.5%); - 81.7 % of women during lactation haveanemia (Hb <70g/L - 7.3%) • 90% adolescentsare also anemic (Teoteja et al 2003) • > 80%childrenyounger than 3 yearsare anemic (NFHS-II& Agarwal et al., 2003)
Anemia criteria (capillary blood) in newborns In newborns of the first and the second weeks of life • Hb < 145 g/L • Hct < 45 % • RBC < 4,5 * 1012/L The third week and fourth weeks of life • Hb < 120 g/L • Hct < 40 % • RBC < 4,0* 1012/L
Normal values of Hb according WHO criteria (capillary blood) : • In infants from 2 to 6 months – > 95 g/L • In children from 6 months to 5 years - > 110 g/L • Elder than 5 years - > 120 g/L
CAUSES OF NEONATAL ANEMIA: 1. BLOOD LOSS (POSTHEMORRHAGIC), the commonest cause of anemia, including: A.Obstetrical causes: placental abruption, placenta previa, trauma to placenta orumbilical cord during delivery and rupture of anomalous placental vessels B.Feto-maternal transfusion: 8% of normalpregnancies have some blood admixture. C.Feto-placental transfusiondue to positioning of infant above level of placentaafter delivery, partial cord occlusion
D. Twin-twin transfusionOccurs only with monochorionic (i.e., monozygotic) twins and when there areplacental vessels which allow shunting of blood from one twin to the other. •Donor will have anemia of variable severity. •Recipient will have polycythemia of variable severity. E. Internal hemorrhagesuch as intracranial hemorrhage, subgaleal hemorrhage,cephalohematoma, adrenal hemorrhage, subcapsular hematoma of liver etc. F. Iatrogenic blood losssecondary to sampling of blood for laboratory tests. This isthe commonest cause of anemia in newborns
2. INCREASED RBC DESTRUCTION (HAEMOLYTIC): A. Intrinsic causes:Hereditary RBC disorders (rare), including: •RBC Enzyme defects (e.g., G6PD deficiency) •RBC membrane defects (e.g., hereditary spherocytosis) •Hemoglobinopathies (e.g., α-thalassemia) B. Extrinsic causes: •Immune hemolysis:-Rh incompatibility, -ABO incompitability, -Minor blood group incompatibility (e.g., Kell, Duffy), -Hemangiomas (Kasabach-Merritt syndrome) •Acquired hemolysis:-Infection, -Vitamin E deficiency (of historical interest, now it is very rare), -Drugs
3. DECREASEDRBC PRODUCTION (HYPOPLASTIC, DEFICIENCY): A.Anemia of prematurity due to transient deficiency of erythropoietin B.Aplastic or hypoplastic anemia (e.g., Diamond-Blackfan) C.Bone marrow suppression (e.g., with Rubella or Parvovirus B19 infection) D.Nutritional anemia (e.g., iron deficiency), usually after neonatal period E. Megaloblastic anemia (B12 and/or folic acid deficiency)
Physiological anemia of infancy • Normal newborn- High Hb level progressively declines by 8-12 wk -9-11g/dl.- Hypoxia stimulates Renal and Hepatic oxygen sensors – erythropoietin production increases. • Preterm- Hb decline is extreme & rapidly falls to 7-9 g/dl by 3-6 wk of age.- Sampling for Lab tests. There are relatively insensitive Hepatic oxygen sensors; as Renal Oxygen sensors switch on at 40 wk of gestation.
CLINICAL FINDINGS IN ANEMIA •Pallor •Tachycardia, tachypnea •Apnea •↑ O2 requirements •Lethargy •Poor feeding •Hepatosplenomegaly (hemolytic disease) •Jaundice •Hypotension •Metabolic acidosis with severe anemia
DIAGNOSTIC EVALUATION OF ANEMIA: 1. History: • Family: Anemia during pregnancy, ethnicity, jaundice in anamnesis • Maternal and perinatal: Blood type and Rh; anemia; complications of labor or delivery • Neonatal: Age of onset; presence of other physical findings
2. Laboratory Evaluation • CBC with platelets, smear and reticulocyte count • Blood group and type, direct antiglobulin test (Coombs test) • Bilirubin (total and indirect) • Kleihauer-Betke Test (on maternal blood to look for fetal red cells as evidence of feto-maternal transfusion) • Ultrasonogram for internal bleeding (head, abdomen) • Rarely, haemoglobin electrophoresis and RBC enzymes • Bone marrow aspiration is exclusively rare necessary to diagnose anemia in a newborn
MentzerIndex • MCV/RBC> 14 = Iron Deficiency • MCV/RBC < 13 = Thalassemia Minor
MANAGEMENT will depend on cause and severity of anemia: • Prenatal: Diagnosis of significant fetal anemia is unusual except in hemolytic disease of the newborn and Parvovirus B-19 infection. Fetal transfusion may be needed for severe anemia.
2. Postnatal: A. Anemia of prematurity:The main methods of management are: •Limit blood taking for laboratory tests •Treatment with recombinant human erythropoietin (r-Hu-EPO), Epoetin - 150 – 200 units/kg subcutaneously three times per week
Indications for transfusion with packed red blood cells (PRBCs) inneonatal anemia Rule № 1. All transfusions that are not strictly indicated are strictly contra-indicated
Indications for transfusion with packed red blood cells (PRBCs) inneonatal anemia • For premature babies: Hb < 70 g/L, Hct < 30 % BUT can be indicated although in higher Hb level (not more than 90 g/L usually) if newborn has is tachycardia > 170 per minute, tachypnea > 60 per minute or cardiomegaly on X-ray only because of anemia (other reasons have to be excluded)
Indications for transfusion with packed red blood cells (PRBCs) inneonatal anemia • For term babies (European Transfusiologists Society, 1998) • Anemia withacuteheart insufficiency - 5 ml/kg slowly during 2-4 hours - repeated transfusions if necessary • Hb < 100 g/L with anemia symptoms (younger than 10 days of life), > 10 days – Hb < 90 g/L • Hb < 130 g/L in severe respiratory diseases • Hb < 130 g/L immediately after birth • > 5-10 % of volume of blood circulation loss
Treatment of hypoplastic anemia • Glucocorticoids (prednisolone 2 mg/kg/day, metipred, solupred – 10 mg/kg/day 3-5 days) • In Fanconi anemia – prednisolone + androgens • Bone marrow transplantation
Megaloblastic Anemia Hypersegmented Neutrophil – 98% had one cell with >6 lobes; Oval macrocytes. Bone-marrow- Large Erythrocyte and Leucocyte series; Megaloblasts have sieve like chromatin- dissociation between nucleus and cytoplasm maturity. Vitamin B12 and folate levels to differentiate.
Peripheral blood smear showing hypersegmented neutrophils, characteristic of megaloblastic anemia.
Treatment of deficiency neonatal anemia • Fe-deficiency: After 1 months of life – combination of iron 3-6 mg/kg in 2 or 3 devided doses for a minimum of 2 months + folic acid 0,4 mg/kg daily Before 1 month only folic acid
Feeding in early infancy • Baby should be breast fed colostrum and mature milk, both have 49% absorbable iron this is sufficient with available fetal stores till baby doubles the birth weight. • Weaning foods from 6 months onwards should have one iron rich dietary item and iron supplementation be given as recommended. Cook in iron vessels.
Iron fortified food. • Iron supplements have been highly effective in fortification trials with Egyptianflat breads, curry powder in South Africa, fish sauce in Thailand, and sugar in Guatemala. • In Grenada , flour used in commercial baking is enriched with iron and B vitamins,. • Indianresearchers have field tested with success iron fortified salt • Pasteurized milk (iron 15 mg/ L and vitamin C 100 mg/L)-is used inGB, USA
Availability of dietary iron by cooking in cast iron utensils: • WHO 1992 prevalence of pregnancy anemia report, records that lowest, rates of all the sub regions of the developing world were observed in southern Africa, due to wide spread use of iron cooking pots by indigenous people. • It was demonstrated that cooking in cast iron utensils, for boiling milk, cooking vegetables etc, provided extra dietary iron. This available dietary iron is well absorbed.