HIV-Related Neuropathy Management with Spinal Cord Stimulation
Learn about using spinal cord stimulation for safe and effective pain management in a case of HIV-related polyneuropathy that didn't respond to traditional treatments.

HIV-Related Neuropathy Management with Spinal Cord Stimulation
E N D
Presentation Transcript
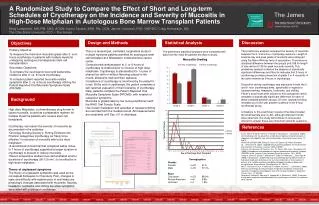
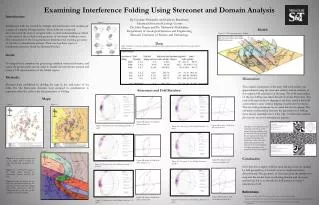
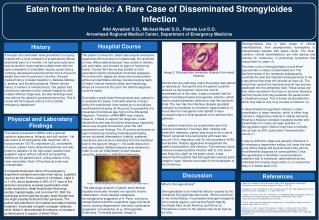
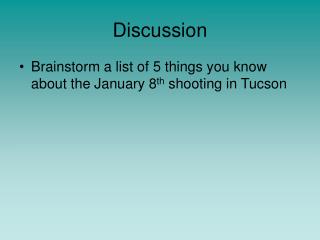
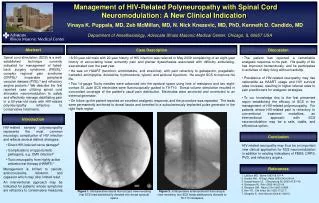
Management of HIV-Related Polyneuropathy with Spinal Cord Neuromodulation: A New Clinical IndicationVinaya K. Puppala, MD, Zeb McMillan, MD, N. Nick Knezevic, MD, PhD, Kenneth D. Candido, MDDepartment of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL 60657 USA Abstract Case Description Discussion Spinal cord stimulation (SCS) is a well-established technique currently indicated for management of failed-back surgery syndrome (FBSS),1 complex regional pain syndrome (CRPS),2 inoperable peripheral vascular disease (PVD),3 and refractory angina pectoris.4We describe the first reported case utilizing spinal cord stimulator neuromodulation to safely and effectively manage debilitating pain in a 50-year-old male with HIV-related polyneuropathy refractory to conservative treatments. • A 50-year-old male with 20-year history of HIV infection was referred in May 2009 complaining of an eight-year history of excruciating lower extremity pain and plantar dysesthesias associated with difficulty ambulating, exacerbated over the past year. • He was on HAART (tenofovir, emtricitabine, and etravirine), with pain refractory to gabapentin, pregabalin, tramadol, amitriptyline, duloxetine, hydrocodone, tylenol, and epidural injections. He sought SCS to improve his life. • Two 14-gauge Touhy needles were advanced into the epidural space using loss of resistance and two eight-contact St. Jude SCS electrodes were fluoroscopically guided to T9-T10. Dorsal column stimulation resulted in concordant coverage of the patient's usual pain distribution. Electrodes were anchored and connected to an external generator. • On follow-up the patient reported an excellent analgesic response, and the procedure was repeated. The leads were permanently anchored to dorsal fascia and tunneled to a subcutaneously-implanted pulse generator in the right flank region. • The patient has reported a remarkable analgesic response to his pain. His quality of life has improved tremendously, and he participates in activities of daily living without hardship. • Prevalence of HIV-related neuropathy may rise nationwide as HAART usage and HIV survival rates increase, resulting in higher referral rates to pain practitioners for analgesic strategies. • To our knowledge this is the first presented report establishing the efficacy of SCS in the management of HIV-related polyneuropathy. For patients whose HIV-related pain is refractory to conventional treatment modalities, an interventional approach with SCS neuromodulation may be a safe, viable, and efficacious option. Introduction • HIV-related sensory polyneuropathy represents the most common neurologic complication of HIV infection and reflects several distinct etiologies: • Direct HIV-induced nerve damage5 • Complications of opportunistic pathogens, e.g. CMV infection6 • Toxic neuropathy from highly-active antiretroviral therapy (HAART)7 • Management is limited to opioids, anticonvulsants, lidoderm, and capsaicin which may offer limited relief. • An interventional approach may be indicated for patients whose symptoms are refractory to conservative measures. Conclusion HIV-related neuropathy may thus be an important new clinical application for SCS neuromodulation in addition to existing indications of FBSS, CRPS, PVD, and refractory angina. References 1. LeDoux MS. Spine 1993;18:191-4. 2. Kemler MA. N Engl J Med 2000;343:618-24. 3. Augustinsson LE. J Neurosurg Sci 2003;47:37-40. 4. Borjesson M. Pain 2008;140:501-8. 5. Simpson DM. Neurol Clin 1992;10:685. 6. Kim YS. Clin Infect Dis 1993;17:32-7. 7. Morgello S. Arch Neurol 2004;61:546-51. Figure 1. Intraoperative lateral fluoroscopic view revealing first SCS lead satisfactorily directed into dorsal epidural space Figure 2. Intraoperative anteroposterior fluoroscopic view revealing two SCS leads satisfactorily directed to T9-T10 interspace