Aspirin, ICDs, and MRA
490 likes | 641 Vues
Aspirin, ICDs, and MRA. Valentin Fuster MD Director, Cardiovascular Institute Mount Sinai Medical Center New York, New York Christopher Cannon MD Cardiologist Brigham and Women's Hospital Boston, Massachusetts James Ferguson MD Associate Director, Cardiology

Aspirin, ICDs, and MRA
E N D
Presentation Transcript
Aspirin, ICDs, and MRA Valentin Fuster MD Director, Cardiovascular Institute Mount Sinai Medical Center New York, New York Christopher Cannon MD Cardiologist Brigham and Women's Hospital Boston, Massachusetts James Ferguson MD Associate Director, Cardiology St Luke's Episcopal Hospital and Texas Heart Institute Houston, Texas Michael Weber MD Professor of Medicine SUNY Downstate College of Medicine Brooklyn, New York
Subjects Aspirin New questions about an old drug MADIT-II ICDs for post-MI patients with low EF MRI Non-invasive assessment of coronary arteries
3 things we know about aspirin • It benefits patients with AMI and unstable angina • It is protective in the long-term for patients with prior MI or stroke • Optimal daily dose is 75 — 325 mg
BMJ meta-analysis Reprinted with permission from BMJ Baigent C et al. BMJ 2002; 324:71-86.
Aspirin for angina? • 60.2-month follow-up of 333 patients with angina and no prior MI from Physicians Health Study Aspirin group: n=178, alternate-day 325mg dosePlacebo group: n=155 Ridker PM et al. Ann Intern Med 1991; 114:835-9.
SAPAT • Swedish Angina Pectoris Aspirin Trial 2035 patients randomized to aspirin (75 mg daily) or placebo Juul-Moller S et al. Lancet 1992;340:1421-5.
BMJ meta-analysis Reprinted with permission from BMJ Baigent C et al. BMJ 2002; 324:71-86.
Underlying diagnoses • The Oxford group has resisted stratifying patients by underlying diagnoses • They prefer to talk about atherosclerotic or occlusive arterial disease • In any circumstance, the use of aspirin is protective • They get a little hostile if you start subdividing Weber
Acute stroke and PAD • Proportional reduction of vascular events Baigent C et al. BMJ 2002; 324:71-86.
A continuum of disease • "The argument that the whole group made […] was that we shouldn't think of vascular disease as regional, but peripheral arterial disease is part of the same continuum." Weber
Meta-analyses • You must focus on the event rates that you are trying to impact. • "That's why I think it's valuable to look at the data from these sort of meta-analyses, to tease out things we might not see in individual trials." • Ferguson
The Physicians study Effect of aspirin on MI and stroke for 22,071 patients with 60.2 months average follow-up N Engl J Med 1989; 321:129-35.
Benefit of aspirin Estimates of benefit of aspirin for patients with various levels of baseline risk for coronary heart disease Hayden M et al. Ann Intern Med 2002; 136:161-72.
Targeting • "You have to look at the mechanistic process that you're targeting, and what you are trying to prevent" • In primary prevention population event rate is low, but the benefit of preventing disease progression may be profound • Risk stratification must be thought about long and hard Ferguson
Weighing the risks of aspirin Estimates of benefit and harm of aspirin for patients with various levels of baseline risk for coronary heart disease Hayden M et al. Ann Intern Med 2002; 136:161-72.
Take home message "[In primary prevention] we need to be a little bit more circumspect before we widely prescribe something that may be associated with some adverse side effects." Ferguson
Aspirin vs statins • Statins: not just preventing acute events, but preventing progression of a remorseless underlying disease • Aspirin: focused on a short-term prevention of acute events • Weber
3 strategies • 3 processes in acute events as targets • In preventive strategy, you aim to reduce likelihood of plaque rupture • If rupture takes place, you try to enhance normal endothelial function • If endothelium is overwhelmed, you focus on aggressive antiplatelet therapy Ferguson
Aspirin responsiveness • Aspirin is not effective in 10-20% of the population according to platelet aggregation studies. • "We have a large population that we are not really protecting." • Fuster
COX inhibitor history • Cox 1 inhibitors block thromboxane release, but can also cause stomach problems • Cox 2 inhibitors protect the stomach, but may block prostacyclin and therefore may be prothrombotic
Cyclo-oxygenase inhibitors and MI • August 2001: MI significantly higher in patients taking either rofecoxib or celecoxib than in placebo patients • -Mukherjee D et al. JAMA 2001; 286:954-959 • November 2001: Higher rate of CV events in rofecoxib patients likely the result of the antiplatelet effects of naproxen • -Konstam MA et al. Circulation 2001;104:2280-8 • January 2002: no evidence that the NSAID, naproxen, is cardioprotective • -Ray WA et al. Lancet 2002;359:118-23
Rofecoxib vs naproxen Relative risk of APTC endpoint in patients taking rofecoxib in comparison to other anti-inflammatory drugs Konstam MA et al. Circulation 2001; 104(19):2280-8.
Cox 2 inhibitors and aspirin • “The lesson is that if you are going to put someone on a cox-2 inhibitor, for goodness sake if that patient deserves to be on low-dose aspirin, they must continue on that treatment.” • Weber
Ibuprofen vs aspirin • Q- “I’m going to take ibuprofen because I know it affects the platelets and maybe it's helping. I cannot take aspirin . . . what would you say? • -Fuster • A- “I would not recommend ibuprofen if they can’t tolerate aspirin, they’re going to get into trouble with that as well. Ibuprofen is not a solution for that problem. • -Weber
The “drug level thing” • Ibuprofen- transient levels of platelet inhibition, peaks and troughs throughout the day • Naproxen- much longer half-life, much higher steady level of platelet inhibition • Diclofenac - least potent, in terms of its cox-1 inhibition • Cannon
GP IIb/IIIa Lessons? • “Certainly the lessons from the IIb/IIIa realm is that dose and level of effective platelet inhibition seem to be important to have clinical efficacy.” • Cannon
Anti-inflammatory vs anti-platelet • “I think it would be really alarmist and totally unwarranted to equate ibuprofen with the oral IIb/IIIa blockers. I think ibuprofen is a great anti-inflammatory drug, but it is not a sustained anti-platelet drug and it may potentially interfere with the anti-platelet effects of aspirin.” • Ferguson
Aspirin effects • Need clinical data on clinical events in patients on aspirin with and without cox 2 inhibitors • Cox 1 effects of aspirin are about 170x greater than their very weak cox 2 effects • Ferguson
MADIT-II • Multicenter Automatic Defibrillator Implantation Trial II • 1232 post-MI patients with moderate LV dysfunction (EF 30%) randomized to ICD or medical therapy • Arrhythmia was not an inclusion criteria
Mortality in MADIT-II 25 20 15 ICD Percent mortality Medical therapy 10 5 0 30% total reduction of mortality
Economic impact • MADIT-II entry criteria would lead to an additional 300,000 patients for ICDs, a $9 billion market • ICDs cost $25-35,000 • "We are dealing with an issue that could have incredible economic implications" • Fuster VENTAK PRIZM 2 ICDSource: Guidant
Mortality in MADIT-II 25 20 15 ICD Percent mortality Medical therapy 10 5 0 30% total reduction of mortality
Risk stratification:MADIT II • Can we find subgroups that have greater or lesser benefit, so that there is some form of risk-stratification? • "Does this have to do with presence of previous bypass surgery? Number of previous infarcts? Or extent of disease?" • Ferguson VENTAK PRIZM 2 ICDSource: Guidant
Steps to implementation First people need to see the data Guidelines for selecting patient populations Incorporation into clinical practice Cannon Vice President Dick CheneySource: GWU hospital
Reduced cost in the future "The hope is that with supply and demand, if there is all of a sudden a huge number of patients eligible for the therapy, the cost will come way down." Cannon
Cost issues "The pharmaceutical industry and the device industry are very different from the world of Bell Telephone which was broken up as a monopoly. I would be surprised if the prices on these things plummet precipitously." Ferguson Bx-Velocity StentSource: Cordis
Cheap ICDs alternative • "For some patients, a sophisticated ICD that could be used to treat comorbidities and monitor a variety of physiological functions may be indicated, whereas in others, an inexpensive ICD in the $10,000 to $15,000 range might be preferable." • Zipes Dr Douglas ZipesSource: Indiana University School of Medicine Zipes DP, Circulation 2001; 103:1372-4.
How long are you prolonging life? • In these sick patients, how much life are we giving them? • "Statistically, we are used to comparing over a short period of time 'A is better than B.' But I think we are going to talk more and more about how much we prolong the life of this individual." Fuster
SCD-HeFT • 2500 patients with either ischemic heart failure or dilated cardiomyopathy in proportions of roughly 50-50, EF 35% • Randomized to 3 arms: ICD, amiodarone, or placebo
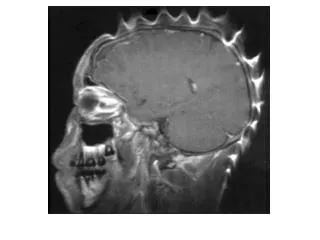
Medical Resonance Angiography • Non-invasive MRI for assessing high-risk patient • MRI of the blood • No contrast agent • A recent study of 109 patients Source: Radiological Society of North America
Coronary MRA results for left main or 3-vessel disease Kim WY et al. N Engl J Med 2001; 345:1863-9.
Limitations of MRA Couldn't adequately image 16% of proximal segments "I have some concerns about that and I am not going to turn all of our cath labs into MRI suites." Ferguson
Straight to the OR? • Q - “If you were to go [MRA] and you found major stenotic lesions… would you now feel bold enough to go straight to the operating room? • -Weber • A - “Personally I would not, because the technique does not image your distal targets all that well. • "If they were my coronary arteries I would want to know what the distal vessels look like that I would be tying into. • -Ferguson
Other imaging technology • MRA technology is advancing rapidly. • "I don't think this technology, regardless of the method you use, is prime time. I think what is very fascinating though, is to see the resolution of this technology just in the last 2-3 years." • Fuster
Questions raised Aspirin Will always be a discussion MADIT-II We have a fantastic therapy, what do we do with it? MRI New diagnostic imaging technologies are evolving rapidly
Applying the evidence • "I'm looking forward to trying to apply all of this evidence, bringing the therapies such as defibrillators […] and aspirin to all the patients who are eligible. I think it can translate into big- time benefits clinically. • Cannon
Risk stratification • "We need to be selective to some extent in what we use and how we use it. We ultimately, with all of the different modalities that we've been coming back to, have come back to issues of risk stratification." Ferguson
Final thoughts on aspirin • "Low-dose aspirin is the way to go with aspirin, in all likelihood for most of our patients." • But you can't give aspirin just because a person reaches a certain milestone age Weber
Aspirin, ICDs, and MRA Valentin Fuster MD Director, Cardiovascular Institute Mount Sinai Medical Center New York, New York Christopher Cannon MD Cardiologist Brigham and Women's Hospital Boston, Massachusetts James Ferguson MD Associate Director, Cardiology St Luke's Episcopal Hospital and Texas Heart Institute Houston, Texas Michael Weber MD Professor of Medicine SUNY Downstate College of Medicine Brooklyn, New York