Download
1 / 21
800 likes | 3.6k Vues
Optiflow TM via Airvo TM High/Low Flow Oxygen Delivery System. Devika Cook Charge Nurse Adult and Emergency PACU Auckland City Hospital. What is the definition of a double blind study?. Two Orthopaedic Surgeons trying to read an ECG!. Objectives. Optiflow TM.

E N D
OptiflowTM via AirvoTMHigh/Low FlowOxygen Delivery System Devika Cook Charge NurseAdult and Emergency PACUAuckland City Hospital
OptiflowTM • Nasal High/Low Flow Oxygen Therapy • Designed to meet inspiratory demand • Provides natural balance of temperature and humidity • Low level positive airway pressure • Used in conjunction with the AirvoTM
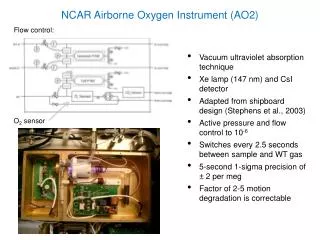
AIRVOTM • High-performance humidifier and integrated flow generator • Consistent temperature & humidity level • Accurate FiO2 with a constant flow rate • Ability to alter flow rate (15-45 lpm and oxygen percentage 21-60%)
Indications for Use • Increased respiratory demand • Intolerance of conventional face mask • Hypoxia/Emergence Agitation • Major surgery – abdominal,head and neck • High BMI • Obesity • Smoker
Benefits • Easy to implement • Comfort → patient compliance • Not affected by NGT • Can prevent less invasive ventilation • Direct Delivery to Naso/Oro-Pharynx • Less dilution effect
Benefits - cont • Warm humidified oxygen • Less damage to mucosa • Improved gas exchange and O2 saturation • Decreased LOS in PACU • Transferable system for ward use • Reduced care costs Disadvantage • No battery pack, dependent on AC power
Case Study • 34 year old male caucasian • Post-Op Lap Appendicectomy • ASA 1 – training for Auckland Marathon • ? Aspirated on induction • CXR – “slight” Pulmonary Oedema • Decreased saturations in PACU
Clinical Presentation • Patient not distressed • Breathing not laboured • Hudson Mask on 15 litres • Persistent low sats 88-90% • Nil complaints of Pain or PONV • Circulation stable • Medical request for CPAP circuit
CPAP Circuit “Dolly Parton”
Treatment • 1400 - OptiflowTM via AirvoTMcommenced • Initially set for high oxygenation • 15 lpm of oxygen (piped via flow meter) • 15 lpm flow rate (generated by AirvoTM) • Approximate oxygen concentration 63% • Arterial line inserted • ABG’s at 30 minute intervals
Treatment - cont • 1500 – sats slight improvement to 92% • 1600 – sats up to 94% • 1630 – commenced weaning of O2 • ↓Oxygen flow 7 lpm(50%) • ↑Flow rate to 30 lpm • Saturations constant in mid 90’s • Constant monitoring of ABG’s & pulse ox • OptiflowTM/AirvoTM titrated for effect
Outcome • Referred to HDU → “wait & see” • Oxygen flow decreased incrementally • Steady improvement in saturations • Re-routing of ward • Six hours later stable • Oxygen flow ↓ 5 lpm • Flow rate maintained at 35 lpm approx 32% • Maintaining saturations at 97-98% • 2000-transferred to Gen Surg ward with OptiflowTM/AirvoTM
Resolution • 24 hours later • CXR Pulmonary Oedema resolved completely • Maintaining adequate saturations on air • 48 hours – discharged home • Unable to complete the Marathon
Conclusion • Early intervention with OptiflowTM/AirvoTM O2 deliveryand humidification does have an impact on patient outcomes • Works relatively quickly – sustained effect • Suitable for patients when conventional masks are not feasible • Can decrease LOS in PACU “Simply Better Oxygen Therapy”
Acknowledgements • Product Specialist F & P • Annelise La Roche • Materials Management ACH • Nurse Educators PACU • Liz Boucher & Penny Jones • Level 8 PACU RN’s • For embracing the technique and ongoing support of the system
The A, B, C of Anaesthesia • Airway • Bagel • Coffee