Download
1 / 30
300 likes | 399 Vues
This briefing material analyzes workforce challenges related to Long Term Neurological Conditions (LTnC) in the East Midlands SHA region. The study identifies key policy shifts and outlines a pathway for MS, PD, and MND, emphasizing early referral, diagnosis, and palliative care. It also presents modeling assumptions, policy levers, and outcomes to inform future workforce strategies.

E N D
East Midlands SHA Next Stage Review – LTnC Modelling the challenge to workforce – briefing material [NOTE: the outputs from the modelling reflected in this presentation material represent work in progress and are subject to ongoing refinements as assumptions are challenged and refined.]
Purpose & context • To identify the ‘challenge to workforce’ arising from key policy shifts identified in ‘From Evidence to Excellence’ for people with selected Long Term neurological Conditions (LTnC); • To undertake this work at an SHA-wide level but with potential and intent to engage with and inform local commissioning; • To undertake the work in such a way as to facilitate debate about future roles, including the contributions made by service users, carers and the wider health and social care ‘market’ in the context of increasing personalisation.
Process adopted • Engagement events with the Clinical Workforce Group to identify key workforce issues; • Reviewed literature and undertaken one-to-one discussions to identify a high level pathway for three LTnC’s; • Undertaken analysis to populate these pathways to provide a quantified profile of needs over time that is sensitive to the key policy changes envisaged in ‘Form Evidence to Excellence; • Met with further engagement group in January 2009 to identify initial detail of activities at each stage of the pathway; • Development and testing of identified pathway activity using both the Health Functional Map (Skills for Health) and the systems model (WSP).
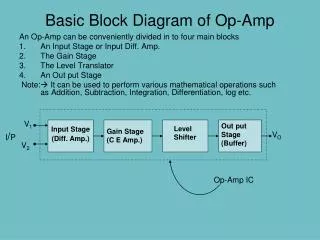
MS pathway & key factors Average life expectancy of 12 years Primary progressive MS Palliative phase 15% (7 pa per 100,000 pop) Onset Diagnosis 85% Relapsing remitting MS Secondary progressive MS 1 – 2 yrs? 50% within 10yrs Early referral Both new ways of working and new treatments will slow down/delay move to progressive condition Referral for symptom management and information prescription New treatments, e.g. Alemtuzumab
PD pathway & key factors Average life expectancy of 17 years Maintenance phase Complex phase Palliative phase (17 pa per 100,000 pop) Onset Diagnosis Slows disease progression 9 – 12 mths? Reduced time to diagnosis brings forward appropriate prescribing and improved care management Early referral Referral for symptom management and information prescription
MND pathway & key factors Average life expectancy of 3½ years Disease mgt Palliation & symptom control (2 pa per 100,000 pop) Onset Diagnosis Recognition To appt Confirmed 18wks or less (4?) Follow-up in 2wks ? Co-ordination Care mgt Palliative care Early referral Fast track appts Care mgt available Awareness
MS: 7 new cases a year giving prevalence of 120 with average life expectancy of c.12yrs. Parkinson’s: 17 new cases a year giving prevalence of 200 with average life expectancy of c.17yrs; Motor Neurone Disease: 2 new cases a year giving prevalence of 7 with average life expectancy of c.3 ½ yrs. Initial conditions modelled (per 100,000 population)
Generic points along the pathway 1) New cases presenting (incidence) 5) People admitted to hospital with a primary diagnosis of LTnC 6) People admitted to hospital with a secondary diagnosis of LTnC 2) Empowering people with low level needs 3a) People transitioning to more complex needs Crisis/acute ‘events’ 3b) People whose needs are complex – care co-ordination 7) People supported at home as an alternative to hospital admission with a primary diagnosis of LTnC Progress of the condition 9) People transitioning to palliative care 8) People supported at home as an alternative to hospital admission with a secondary diagnosis of LTnC 4) Supporting people with palliative needs 10) Last days of life
Key policy levers or changes • The overall impact of demographic changes on the incidence and prevalence of the 3 conditions; • The impact of providing support at the early stages of diagnosis and enhancing self care such that the period before complex care management is needed is extended; • Avoiding significant numbers of hospital admissions and providing care through integrated and co-ordinated specialist teams for people at home; • Supporting choice at the end of life resulting in fewer people dying in hospital.
Modelling assumptions • Early intervention increases the time people have before their needs become complex and they need care management input by 6 months; • There is a reduction in people dying in hospital rather than at home from 65% to 40%; • 20% of current admissions for a secondary condition are cared for at home and 40% of those admitted to hospital with a primary LTnC condition are also cared for at home.
Model demonstration • Incidence and prevalence across the East Midlands: • Baseline; • With demographic change; • With policy levers switched on. • Outputs demonstrating: • Change in overall needs due to demographic changes and therefore total workforce; • Skill mix: generic/enhanced/specialist; • Shifting balance between hospital and home.
Scaling the service (demographic impact only) – total service (community & hospital) • East Midlands PCTs typically c.250,000 for a city (Derby, Leicester and Nottingham) and c.700,000 for Counties; • Total population of East Midlands at c.4,400,000 so (without adjustment for differential levels of need apart from straightforward population split) indicative capacity requirements are:
Scaling the service • Skill mix: • 28% generic tasks; • 44% enhanced; • 28% specialist. • Change through demographic impact (10 year horizon): • 5% increase for generic and specialist skills; • 9% increase for enhanced skills.
Hospital admissions • Illustrative based on either a ‘city’/county configuration with population of 950,000 or a ‘town’/county configuration with a population of 700,000, indicative capacity requirements are:
Hospital staff • Skill mix: • 21% generic skills; • 63% enhanced; • 16% specialist. • Proportion of total skills supporting acute admissions: • 42% of generic skills; • 80% of enhanced skills; • 33% of specialist skills.
Comparison of skill mix Hospital: Community:
Impact of policy levers • Has the effect of shifting the emphasis: • From complex to maintenance levels through early intervention; • From the hospital to the community by providing alternatives to admission. • How does this work through to skill mix and the development of MDT community teams?
Early intervention impact • Supporting people for longer at the ‘maintenance’ level through early intervention:
Shift of hospital activity • Admissions diverted through enhanced community MDT working:
Scaling the service with policy impact – total service (community & hospital) • Overall workforce remains broadly level (i.e. Policy shifts have cancelled out increased incidence due to aging population), hence indicative capacity requirements are:
High level changes in skill mix • Overall impact is to increase qualified workforce (particularly in the community – see later slides):
Change in hospital staffing • Overall reduction/shift to the community of c.17% from initial indicative capacity requirements, but minimal impact on skills mix: 2008 to 2018
Change in community staffing • Overall increase/shift to the community of c.20% from initial indicative capacity requirements, and significant impact on skills mix: 2008 to 2018
Workforce shifts • If services were staffed in line with the initial indicative capacity requirements (recognising that this will rarely be the case, particularly in the community) then over a 10 year period, in response to both demographic and policy changes, there would be across the E Midlands: • 21wte less generic capacity required in hospitals – with the need for 3wte more in the community (a ‘surplus’ of 18 wte); • 59wte less enhanced capacity required in hospitals – with the need for 96wte more in the community (a ‘deficit’ of 37wte); • 13wte less specialist capacity in the hospitals – and 13wte too much in the community (a ‘surplus’ of 26wte).
The ‘team’ • Model outputs identify those whose time will be required to input at the different stages, but this will include input by members of other teams, for example GP’s or the acute sector workforce; • It is therefore necessary to map the functions and activities (and therefore workforce requirements) against a local service model: • What is the scope of the teams remit? • How does it interface with primary care? • How does it interface with secondary care – is it an outreach or in-reach model?
The current workforce • The modelling identifies an indicative capacity at different skills level based on need rather than what is there now; • It has the potential to be used as a ‘benchmark’ for local discussion and gap analysis that will therefore be more sensitive to the history and opportunities in a locality.
Ongoing refinement • Further iteration of confirm and challenge of the underlying assumptions derived by Skills for Health from the January workshop with a group of professionals; • Updating of the systems model as necessary as a result of the above; • Presentation of the work to the Clinical Advisory Group; • Consideration of cascade to local commissioning and workforce leads.