Download
1 / 19
200 likes | 353 Vues
This document explores the principles of tribal self-governance, including federal programs like direct services from IHS and BIA, and options like 638 contracting and self-governance agreements. It traces the historical context of Indian self-determination from the 1970s to current practices that empower tribes, improve fiscal accountability, and enhance service delivery for community needs. Through examples like the Choctaw Nation's clinics, it illustrates effective management under self-governance and highlights the importance of treating tribes as sovereign entities.

E N D
Tribal Government Services3 Options for Delivery from IHS and BIA • Direct Services: IHS & BIA provide all services through federal employees and facilities • “638 Contracting:” Tribe signs Program Contracts with BIA or IHS to deliver specific programs through tribal departments. (Self-Administration) • Self-Governance: Compact and Funding Agreement with ability to redesign programs and services as well as reallocate funds to meet community need. (Expanded Block Grant)
History of Self-Governance In 1970, President Richard Nixon delivered a message to Congress on “Indian Affairs” in which he laid the groundwork for a change in federal Indian policy from “termination and assimilation” to Indian Self-Determination. • Title I, Public Law 93-638—Authorized the contracting of programs to Tribes-- 1975 • Title II, Title III, Public Law 100-472 & Public Law 102-184 Demonstration for BIA & IHS-- 1988 • Title IV, Public Law 103-413 Permanent BIA-- 1994 • Title V, HR 1167—Permanently established Tribal Self-Governance for IHS-- 2000 • Title VI, Feasibility Study for other DHHS Programs-- 2000
Self-Governance • Definition: A Federal process of Tribal control made possible through Congressional authorization and appropriation support (P.L. 93-638) • Definition: Tribal control and decision making with effective governing institutions– practical sovereignty
Reasons for Self-Governance • Establish better fiscal accountability through expanded Tribal Governmental decision making authority • Institute administrative cost-efficiencies through reduced bureaucratic burdens and streamline decision-making authority • Change roles of the Federal Departments and agencies serving Indian Tribes by shifting their responsibilities from day-to-day management of Tribal affairs to that of Protectors and Advocate of Tribal interests • Improve the quality & quantity of services provided to tribal members • Recognize Tribe’s right to determine priorities, redesign and create new programs to meet local needs • Formalize relations between the United States and Indian Tribes on government-to-government basis as provided for in the US Constitution • Promote greater social, economic, political, cultural stability and self-sufficiency among Indian tribes
Self-Governance: What is it? • The exercise of sovereignty (genuine decision-making power) • Empowerment • Self-Reliance • Self-Sufficiency • Responsibility • Accountability • Self-Governance is a way of life, it is an ongoing process • What it is not: • Dependency • Federal dominance • Paternalism and Control • Not another Federal Program
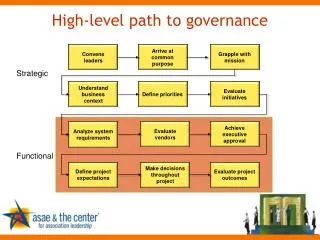
Tribal Management Under Self-Governance • Federal Control Tribal Control $$$ • Advance Lump Sum Payments • Recurring Base Budgets Flexibility • Ability to redesign programs • Ability to merge and assign program funds • Ability to adopt revised regulations Changes Focus of Program Design/Deliver • Community-Driven • Needs-Driven • Priority-Driven Changes Mentality of Tribal Gov’t • Outcomes versus jobs • Long-term planning • Collaboration between tribal dept. • Collaboration between tribe and other governmental entities
THE CHOCTAW NATION OF OKLAHOMA
Atoka Clinic About the Facility Year Built: 2008 Last Remodel: None Square Footage: 11,892 About the Staff Staff Members: 14 (not including medical staff) Medical Staff : MD or DO: 1 DPM: Shared with 0.25 Idabel and Hugo Mid-level Providers 1
Broken Bow Clinic About the Facility Year Built: 2007 Last Remodel: None Square Footage: 6,281 About the Staff Staff Members: 6 (not including medical staff) Medical Staff : Mid-level Provider: 1
Hugo Clinic About the Facility Year Built: 1977 Last Remodel: In Progress Square Footage: 8,964 About the Staff Staff Members: 21 (not including medical staff) Medical Staff : MD or DO 2 DDS 1 DPM: Shared with 0.25 Idabel and Atoka Mid-level Providers 1
Idabel Clinic About the Staff Staff Members: 60 (not including medical staff) Medical Staff : MD or DO 4 DPM: Shared with 0.25 Hugo and Atoka OD 2 DDS 2 Mid-level Providers 1 About the Facility Year Built: 2005 Last Remodel: None Square Footage: 54,546
McAlester Clinic About the Staff Staff Members: 52 (not including medical staff) Medical Staff : MD or DO 4 OD 1 DDS 2 Mid-level Providers 1 About the Facility Year Built: 2007 Last Remodel: None Square Footage: 44,807
Poteau Clinic About the Staff Staff Members: 52 (not including medical staff) Medical Staff : MD or DO 3 DDS 2 Mid-level Providers 2 About the Facility Year Built: 1995 Last Remodel: 2007 Square Footage: 30,754 Poteau Clinic is the home of the CNHSA Pharmacy Refill Center.
Stigler Clinic About the Facility Year Built: 2004 Last Remodel: 2005 (New Addition) Square Footage: 11,120 About the Staff Staff Members: 13 (not including medical staff) Medical Staff : MD or DO 1 OD 1 Mid-level Providers 1
Choctaw Nation Hospital About the Facility Year Built: 1999 Last Remodel: Ongoing Square Footage: CNHCC - 155,580 DWC - 14,760 About the Staff Staff Members: 494 (not including medical staff) Medical Staff : MD or DO 39 DPM 2 OD 2 DDS 3 Mid-level Providers 16