Download
1 / 25
260 likes | 470 Vues
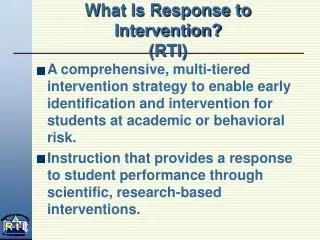
Strategic Plan: Early Identification & Intervention. Improve communication to providers to prevent duplicative testing & Decrease the amount of time it takes between screening and evaluation.

E N D
Strategic Plan: Early Identification & Intervention Improve communication to providers to prevent duplicative testing & Decrease the amount of time it takes between screening and evaluation • Conducted Two Quality Improvement Projects (in multiple locations) linking developmental pediatricians and CDS sites. • Evaluated processes for referral and evaluation, and field tested algorithm to streamline evaluation and access to early intervention Services.
Southern Maine This region’s Early Childhood Interventionists and Diagnosticians had a 10-year contracted relationship that was considered a “highly successful system of referral and evaluation.” Both entities highly respected each others work and appreciated the relationship.
Method: Southern Maine • Adjustment of information CDS includes with referrals. • CDS Case Manager distributes required forms to the family and provides needed assistance in filling them out. • Upon referral, Diagnostician creates an evaluation plan that includes anticipated appointment dates. • Communication of meeting schedule to CDS case manager. • Developed a comprehensive tracking database. • Following joint planning meetings, any medically necessary recommendations that do not have a plan-of-care through the educational system will be documented and sent to the PCP for follow-up through referrals.
Results:Southern Maine • 112 Children Benefited From Quality Improvement Activities (29 Referrals from PCPs and 83 from CDS) • Improved information included on referrals, providing more specifics about the child’s issuesand symptoms • Families are now more aware that there is a concern that their child may have an ASD. Families come in evaluations more thoughtful and informed • Reduced number of “no-shows” • Increased number of families completing paper work in advance of appointments.
Average # Days Between Referral and Final Diagnosis Southern Maine QI activities reduced process by over one month
Northern Maine This regions Early Childhood Interventionists and Diagnosticians had a long history of significant discord and distrust.
Method:Northern Maine • Develop and implement process to identify young children who are in both systems • Communicate timeline for evaluation and reports completed to prevent duplicative assessments • Once evaluation of patient is complete, meet with CDS to discuss a plan that will most likely include a combination of CDS, or educational services, as well as other medical service needed to provide the child a comprehensive early intervention plan.
Results:NorthernMaine • 30 Children benefited from Quality Improvement Activities (All referred by PCPs) • Data was only collected about children who were ultimately diagnosed with ASD • Waiting for Evaluators’ report on pre- and post- interviews • By conducting monthly meetings between clinicians and CDS staff representing both Part B and Part C services, there has been an increased understanding of the processes each agency uses, how they overlap, and how they differ • Able to have productive open conversations between the two entities and physicians have expressed an increased sense of collaboration • Both physicians and CDS have committed to continue meeting after pilot is done
As a community, we have attained a better working relationship among CDS, EMMC, case management agencies, and Section 28 providers. Unfortunately, this remains a very difficult system for parents (and clinicians) to understand and can continue to lead to controversy.
# Days Comparison of Northern and Southern Timeline for PCP Referrals
Age at Diagnosis Comparison National National averages released May 2012 through the CDC (http://www.cdc.gov/nchs/data/databriefs/db97.pdf)
Medical Home Pilot Implement the National Medical Home Autism Initiative recommendations to provide enhanced care coordination services in the medical home for children and youth with ASDs.
Autism Care Management: Husson Pediatrics Michael Ross M.D. Lead Physician and Project Manager, Husson Pediatrics Rochelle Harriman, RN Autism Care Manager
Staffing • 8 FT and PT Providers (MD, DO and FNP) • 3 Triage Nurses (RN) • 5 Clerical staff • 2 Referral/Insurance/Coding Specialists • 7 Physician Extender (Medical Assistants) • 2 Case Managers (Autism and Asthma) • 1 Quality LPN (floating to PE and triage)
Background In 2008-2010, Husson Pediatrics implemented early screening for Autism Spectrum Disorder as part of the ASD Systems Change Initiative While Husson Pediatrics found an increase in diagnostic accuracy, the major barrier to effective care was a lack of care coordination for children with ASD
Measurement Qualitative Interviews Pediatric Impressions Parent Survey Medical Home Care Coordination Measurement Tool
General Impressions • The current system of treatment for Autism Spectrum Disorder in Maine is both confusing and unwieldy. • Parents are not intuitively knowledgeable about what services are available and what services are covered by the medical and educational models. • There is an increased awareness among parents about the role of a case manager as a guide through this difficult and confusing landscape of treatment. • Parents most often sought out care management services upon initial diagnosis and during periods of crisis.
Challenges: In the way Autism care is delivered • Difficulty making contact with outside agencies/service providers • Delay from diagnosis to intervention due to the bureaucracy associated with in processing insurance applications (Maine Care) • Overall disorganization: Missing evaluations, breakdown in communications between agencies (unclear who is doing what). • Maine Care Section 28 provided only services for self-contained programs (special purpose). • Other physicians/practices not willing/prepared to receive older patients with ASD after they turn 18.
Enhanced and Expedited Delivery of Care • Successfully enrolled and enriched the lives of 32 patients and their families. • Children with ASD are enrolled in Medicaid sooner and have access to the medical model of care faster. • Timelines and organization have improved resulting in more timely referrals for external case management, occupational therapy, speech, evaluations, support groups, parent support contacts, schooling, and other services. • Earlier identification of medical issues
Serving the emotionalneeds of patients and families • Parents are feeling supported and validated. • Solutions to behavior issues are discussed by phone, troubleshooting takes place and parents have options and approaches that are immediately implemented. • Establishment of a “support network” of parents with children with ASD who volunteer to talk about issues, concerns and feelings and generally provide emotional support to other parents of children diagnosed with ASD.
Successes: Enhancement of Husson Pediatrics' care of children with Autism • Development of a Husson Pediatrics Office Visit “social story” for the practice web site and Facebook page. • https://www.facebook.com/media/set/?set=a.391443920975412.1073741825.229560353830437&type=3 • Increased awareness of care coordination services in the practice and in the community via outreach and publicity. • Increased provider awareness of available resources. • Increased provider awareness of the importance of Early Identification and Early Intervention.
Future Goals: • Increasing awareness and availability of care management • Continuing to Make Husson Pediatrics ASD friendly • PECS (Picture Exchange Communication System) • Creating social stories to address specific office visits • ENT checks • Weight • Blood Pressure cuffs • Stethoscope • Sustainability • Increase staff awareness of the resources available from the ASD care manager • Potential adoption by ACO