Download
1 / 39
390 likes | 491 Vues
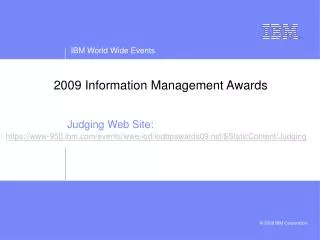
2009 Pandemic Influenza A (H1N1): Our experience this spring, and expectations and planning for the fall. Society for Information Management September 10, 2009. MMWR 2009 Epub April 24. Laboratory confirmed cases of novel H1N1 influenza, Mexico, April and May 2009.

E N D
2009 Pandemic Influenza A (H1N1):Our experience this spring, and expectations and planning for the fall Society for Information Management September 10, 2009
Laboratory confirmed cases of novel H1N1 influenza, Mexico, April and May 2009 MMWR June 5, 2009 / 58(21);585-589
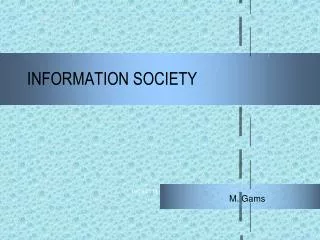
Died 50-75%?? Hospitalized Moderately sensitive Very non specific Medically attended ILI Very Poor Model based ILI cared for at home Asymptomatic persons Surveillance ParadigmEstimation of Influenza Morbidity and Mortality Accuracy 80—90%
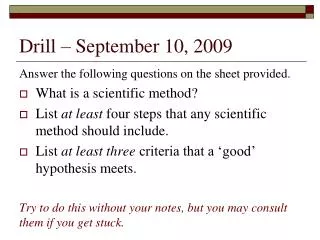
Origins of Novel H1N1 R. J. Garten et al., Science 325, 197 -201 (2009) R. J. Garten et al., Science 325, 197 -201
Utah’s Story • First case reported on 4/28/2009 (onset 4/22) • Cluster in Summit County school children • Travel to Mexico for spring break • Other isolated cases throughout the state • Clusters of illness • Wasatch Front Outbreak
Age specific rates of hospitalization, novel influenza A and seasonal influenza, Utah
Southern Hemisphere Australia- May 8 New Zealand- April 25 South Africa – June 24
Expectations for Fall “Prediction is very difficult, especially about the future”-Niels Bohr, Quantum physicist“If you’ve seen one flu epidemic, you’ve seen one flu epidemic”-Nancy Cox, Influenza Division Chief, CDC
Expectations for Fall • What we know • NYC study estimates 7% of population was infected • New Zealand estimates 11% of population was infected • Pandemic planning and mathematical models estimate 20-40% of population may be infected • Pandemics historically occur in waves • Severity: not 1918 picture, but healthcare system was stressed this spring: • Emergency Departments and ICUs • Homeless clinics and shelters
1918 Influenza PandemicDeath rates - United Kingdom, 1918-19 Tauberberger JK, Morens DM. 1918 Influenza: the Mother of All Pandemics. EID 206;12(1). http://www.cdc.gov/ncidod/eid/vol12no01/05-0979.htm#Figure1
Expectations for Fall • What we don’t know • Will there be a change in severity? • Will there be a change in transmissibility? • Will the upcoming flu season be limited to pandemic H1N1, or include seasonal influenza viruses? • Will Utah’s experience this spring will decrease impact this fall/winter? • Will vaccine be available in time?
Surveillance Plan • Key to understanding: • Onset • Severity • Risk groups • Outpatient rates of influenza-like illness (ILI) • Hospitalizations • Pneumonia and Influenza deaths • School and workplace absenteeism
Viral Testing • Utah Public Health Laboratory • Balance capacity with need for situational awareness • Inform community mitigation efforts • Clinical management • Monitor for genetic drift • Monitor for antiviral resistance
Antiviral Medications • Priority groups: • Hospitalized patients • High risk individuals: • Children < 5 years old • Adults > 65 years of age • Pregnant women • Persons with the following conditions: • Chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic, hematological (including sickle cell disease), neurologic, neuromuscular, or metabolic disorders (including diabetes mellitus); • Immunosuppression, including that caused by medications or by HIV; • Persons younger than 19 years of age who are receiving long-term aspirin therapy, because of an increased risk for Reye syndrome. • Focus on treatment vs. prophylaxis • Early initiation • Use of Stockpile • Monitoring market supply • Uninsured?
Influenza Vaccination • Two flu vaccines this year: • Typical seasonal vaccine- available now! • Pandemic H1N1 vaccine- in production with clinical trials ongoing • Anticipate first shipment of pandemic vaccine to Utah in mid October • May require 2 doses for some or all age groups • Priority groups: • Pregnant women • People who live with or care for children younger than 6 months of age • Healthcare and emergency medical services personnel • Persons between the ages of 6 months and 24 years old • People ages of 25 through 64 years of age who are at higher risk for 2009 H1N1 because of chronic health disorders or compromised immune systems
Vaccine • Distribution and Delivery • Public Health System • Plan varies by jurisdiction • Mass vaccination clinics • Schools • Hospitals and clinics • Challenges • Pregnant women and people ages 25-64 • Mismatch of supply and demand • Risk of adverse events, perceived risks • Logistics: delivery of large number of doses in short period of time
Community Mitigation • Non-pharmaceutical efforts designed to limit the impact of an influenza pandemic on the community at large by minimizing the transmission of influenza • Hygiene • Isolation of ill persons (in home) • Quarantine of household contacts • Community social distancing • Cancelling mass gatherings & closing public places • Workplace social distancing • Excluding ill workers, reducing face-to-face contact • School dismissal
Hygiene • Wash hands frequently with soap and water or use an alcohol based hand cleaner when soap and water are not available • Cover your mouth and nose with a tissue when coughing or sneezing • Avoid touching your eyes, nose and mouth • Avoid close contact (i.e. being within about 6 feet) with persons with influenza like illness
Use of Facemasks and Respirators Adapted from CDC Interim Recommendations for Facemask and Respirator Use to Reduce Novel Influenza A (H1N1) Virus Transmission
Isolation • People with influenza should remain at home until at least 24 hours after they are free of fever without use of fever-reducing medications • Change from previous recommendation of “7 days after illness onset or until 24 hours after resolution of symptoms, whichever is longer” • Most people in the spring had fever for 2-4 days • Does not apply to healthcare workers
Quarantine • Quarantine of household contacts of ill persons is not recommended at this time • Household contacts should monitor their health every day, and take everyday precautions including hand washing and respirator etiquette • If they become ill, they should stay home.
Community Social Distancing • Closure of public places and cancellation of public gatherings are not anticipated for the 2009-2010 influenza season • Some organization may choose to modify customs or practices, as they would in a typical influenza season
Workplace Social Distancing- Current Recommendations - • Advise ill workers to stay home, send home workers that become ill during the day • Flexible leave policies • Ill workers • Caretakers • School dismissal, child care center closure • Do not require doctor’s note for validation of illness or return to work • Recommendations may change if severity of illness changes
Workplace Social Distancing- Increased Severity Compared to Spring 2009 - • Consider active screening of employees • Consider having high risk employees telecommute, reassigned to duties with less person to person contact, or stay home • Consider typical social distancing measures for all employees • Increase physical distance between employees • Telecommuting • Staggered shifts
School Dismissal • Selective school dismissal • School where many or all students are high risk • Excessive absenteeism • Recommendations may change if severity of illness changes • Change “perfect” attendance awards
Communication • Bi-weekly situations reports, surveillance reports, regularly updated guidance materials http://health.utah.gov/h1n1 • Media campaign in development • Press releases and press conferences • Balance overload and fatigue with need to disseminate critical information
Appropriate use of healthcare system • Limit stress on healthcare system while assuring that high risk individuals will seek care early • Even relatively mild outbreak this spring stressed ED’s – too many people who didn’t need ED care sought it • Some of the sickest ICU patients were those who failed to obtain timely care including antiviral medications
Rachel Herlihy, MD, MPH Deputy State Epidemiologist Utah Department of Health rherlihy@utah.gov 1-888-EPI-UTAH (24/7)