Download
1 / 12
140 likes | 445 Vues
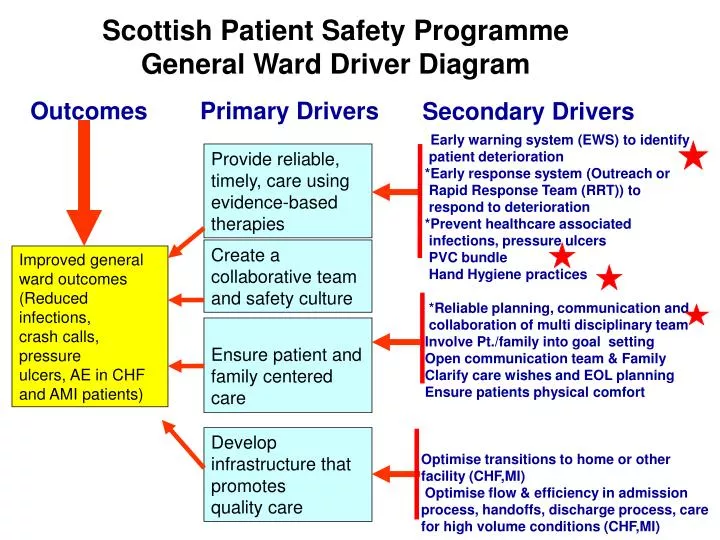
Scottish Patient Safety Programme General Ward Driver Diagram. Outcomes. Primary Drivers. Secondary Drivers. * Early warning system (EWS) to identify patient deterioration *Early response system (Outreach or Rapid Response Team (RRT)) to respond to deterioration

E N D
Scottish Patient Safety Programme General Ward Driver Diagram Outcomes Primary Drivers Secondary Drivers *Early warning system (EWS) to identify patient deterioration *Early response system (Outreach or Rapid Response Team (RRT)) to respond to deterioration *Prevent healthcare associated infections, pressure ulcers PVC bundle Hand Hygiene practices *Reliable planning, communication and collaboration of multi disciplinary team Involve Pt./family into goal setting Open communication team & Family Clarify care wishes and EOL planning Ensure patients physical comfort Optimise transitions to home or other facility (CHF,MI) Optimise flow & efficiency in admission process, handoffs, discharge process, care for high volume conditions (CHF,MI) Provide reliable, timely, care using evidence-based therapies Create a collaborative team and safety culture Improved general ward outcomes (Reduced infections, crash calls, pressure ulcers, AE in CHF and AMI patients) Ensure patient and family centered care Develop infrastructure that promotes quality care
PVC Bundle, Orthopaedic Ward - PDSA Cycle Implement PVC Bundle all Wd 16 patients Ninewells Hospital 95% compliance with PVC Bundle Process by Dec 2009 Adapt and test existing PVC Bundle process carried out within ward 16 to align with SPSP PVC Bundle DATA Implementation of PVC bundle process and audit tool Continue to test process and accompanying audit documentation with all patients and involving all staff to ensure all issues are discovered and resolved Further adaptation of process, test with 3-5 patients and 3 nurses, parallel testing of locally developed audit tool to suit revised process. Test SPSP PVC Bundle within orthopaedic clinical setting with one patient and one nurse. PVC maintenance was already carried out within this Major Joint Replacement Orthopaedic Ward. Testing was required around the implementation of the SPSP Bundle which differed slightly.
SEWS, Angus Community Hospital - PDSA Cycle Implement SEWS Chart Brechin GP Ward 95% compliance with SEWS and early identification of patient deterioration Adapt and test existing SEWS process from other areas to suit within Community Hospital e.g. local algorithm Tested SEWS chart on staff redeployed from local ward that provide cover DATA Tested Algorithm with one call to Out of Hours service Revised Algorithm then further testing with 3 then 5 patients and revised protocol with staff to ensure chart fit for purpose Test suitability of SEWS Chart within Community Hospital with one patient by one nurse
Safety Briefings, Perth Community Hospital - PDSA Cycle Implement daily Safety Briefings within St Margaret's Community Hospital 95% compliance with Safety Briefings including Multi Disciplinary Team (MDT) Adapt and test existing Safety Briefing process from other areas to suit within Community Hospital *100% compliance with Safety Briefings since April 2008* MDT now fully engaging with Safety Briefings, including GPs. Fully implemented reliable process DATA Test that members of the MDT are aware of White Board and importance information displayed Test that staff on each shift check and initial White Board ensuring compliance Test that new safety issues are appropriately added to White Board Test staff awareness of new system (White Board) of where to locate and read safety notices
GENERAL WARDKEYS TO SUCCESS IMPLEMENTING A PVC BUNDLE IN WARD 16 NW Replacing the existing documentation currently in use within ward 16 regarding PVC post insertion care with the SPSP PVC Bundle would allow for a uniform NHST wide format. The documentation previously in use on the ward had been developed due to high risks of HAIs and their impact because of the type of surgery delivered within ward 16. Initial testing looked at the suitability of the new bundle for use within the ward and in particular the Integrated Care Pathway (ICP) currently utilised within the ward. This was initially done with one patient and one nurse before being tried with 5 patients and 3 nurses. Testing was done to ensure all staff were aware of the planned change of documentation within the ICP before implementing across the entire ward. Compliance and how data was gathered was then tested to ensure reliability of the information being gathered and that compliance rates were being met.
GENERAL WARDKEYS TO SUCCESS IMPLEMENTING DAILY SAFETY BREIFINGS WITHIN St MARGARETS COMMUNITY HOSPITAL Daily electronic handovers were already part of the nursing culture, however to increase the reliability and increase dissemination of the information the Senior Charge Nurse wanted to introduce a system that would involve all of the Multi Disciplinary Team, support staff and GPs. A white board was placed within the nursing office with relevant, concise and precise details written upon it. Awareness systems were conducted to ensure with all staff as to how the system would be implemented and maintained. The first test involved ensuring that all the appropriate safety issues were visible. Subsequently testing was carried out around the updating of information on the board. Relevance etc. Compliance was tested next by asking all staff on a shift by shift basis to initial that they had read and understood the information on the board. This was further supported by identifying two champions who further tested that information continued to be updated and that all staff were initialling that they had read the board. The next test involved rolling out the process to all the support staff and members of the MDT. To ensure that the safety issues were relevant spot audits were carried out by the designated champions
GENERAL WARDKEYS TO SUCCESS IMPLEMENTING SEWS CHART IN GP WARD BRECHIN SEWS charts are now an integral component of how care is delivered within the Acute setting, its integration within the community hospital setting is seen as the next logical step. Education for the staff around use of and background to the development and use of SEWS was the first part of process. After testing with one patient and one nurse it was noted that the algorithm used within the acute setting did not suit the environment and conditions found within the community hospital setting. The algorithm was reviewed and revised by staff and then further testing was undertaken with the new format with 3 patients and 3 nurses. Further discussion with staff around implementing SEWS chart throughout the ward highlighted pockets of limited knowledge and lack of confidence with using SEWS across the ward. Further targeted training and education addressed this issue and SEWS were implemented across the ward. With HCA’s an integral part of care provision delivery within the ward, they were trained in a similar fashion to the qualified staff in the use of SEWS charts including determining criteria as to how and when to notify qualified staff of any changes in a patients SEWS score. Staff from local wards often assist on the GP ward and using lessons learned from the process of introducing SEWS training of likely relief is presently being undertaken.
GENERAL WARDKEYS TO SUCCESS HAND HYGIENE: Wd 5 RVH Good hand hygiene was recognised as being a vital component in preventing the contracting and spreading of SABs and HAIs within any clinical setting. The first step undertaken within the ward was testing the staff’s existing knowledge around infection control and hand hygiene in particular. This involved the Infection Control team who also delivered education for all of the ward staff around this area. Testing of the observation tool used in auditing of Hand Hygiene opportunities highlighted that there was not a uniform understanding of what represented and ‘opportunity’. Further education and clarification on the tool itself eliminated this as an issue. Further testing of the audit tool threw up discrepancies in hand washing techniques used by staff underlining that current best practice was not being used 100% of the time which could affect both effectiveness and in measuring compliance. Again education was undertaken around current best practice and estates where asked to replace any taps at the sinks that required staff to touch with just washed hands. Run charts demonstrate that compliance is meeting the minimum standard within the ward and that C-diff rates have been positively affected.
GENERAL WARD PROCESS MEASURES Safety briefings not taking place at weekends Safety briefing board implemented Safety issues included on nurse handover sheet Testing of algorithm of acute services Staff unfamiliar with use of SEWS Dec onwards – ward merged with annexe to become Inpatient Unit – SEWS training to be undertaken with new staff
GENERAL WARD PROCESS MEASURES Audit tool tested Staff education in hygiene provided by infection control Staff issues resulted in deployment of relief staff unfamiliar with surrounding Dressing not dated Dressing not dated Dressing not dated Dressings not dated