Download
1 / 25
250 likes | 404 Vues
WHO comparative evaluation of serologic assays for Chagas disease. Journal Club April 2, 2009. Chagas disease (American trypanosomiasis). caused by the parasite Trypanosoma cruzi, which is transmitted: By the triatomine bug (kissing or reduviid bug) Vertically Blood transfusions

E N D
WHO comparative evaluation of serologic assays for Chagas disease Journal Club April 2, 2009
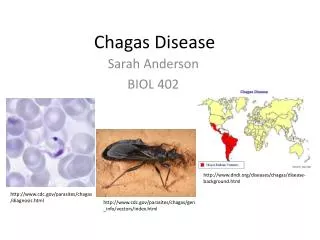
Chagas disease(American trypanosomiasis) • caused by the parasite Trypanosoma cruzi, which is transmitted: • By the triatomine bug (kissing or reduviid bug) • Vertically • Blood transfusions • Organ transplants http://www.cdfound.to.it/img/tryp3.jpg http://www.rso.cornell.edu/bugclub/images/Triatoma%20sanguisuga.jpg
Epidemiology • Endemic in Mexico, Central and South America • 8-11 million people are infected • 45,000 fatalities may occur annually • Those living in rural areas at highest risk (triatomine bugs love mud walls and thatched roofs) • In the US and Canada, infection is increasing as a result of the immigration of infected individuals from endemic areas http://www.aabb.org/Content/Members_Area/Association_Bulletins/ab06-08.htm
Transfusion relevence • Acute, vector-borne infections are mostly mild • Chronic, asymptomatic infection results • acute infection in patients with compromised immune systems can be very serious • It has been estimated that there may be as many as 100,000 legal immigrants in the US and Canada who are unknowingly infected • The rate of seropositive blood donors in the US ranges from 1 in 5400 to 1 in 25,000 • Among high risk populations in Washington and California, the prevalence was 1 in 500, which 20% able to transmit infection • 2 cases of TT-Chagas disease have been identified in Canada http://www.aabb.org/Content/Members_Area/Association_Bulletins/ab06-08.htm http://www.cmaj.ca/cgi/reprint/177/3/242-a
Screening • In 2006, the US FDA approved a serologic enzyme-linked immunosorbent assay (ELISA) for screening donations • Ortho-Clinical Diagnostics
Challenges • Laboratory diagnosis of Chagas disease is challenging • Direct detection of the parasites is difficult • Low parasitemia during chronic phase • Hence, the laboratory diagnosis is based on serologic assays • i.e. looking for T. cruzi antibodies with a lysate of epimastigotes grown in liquid culture • There is no accepted/accessible gold standard • New assays are validated using high-antibody-titre, consensus positive specimens (and thus their ability to detect low-antibody-titre cases is untested) • Sensitivity is overestimated
Purpose • Evaluation of commercially available test kits for Chagas disease for use in blood bank screening is difficult • Lack of large and well-characterized panels • Collaborate effort of Latin American blood centres and the WHO to establish a Chagas disease panel
Design • 437 specimens (Chagas positive and Chagas negative) were provided in 2000 to the WHO Collaborating Centre in San Paulo • 10 Latin American blood centres in 10 countries • Specimens were assigned a positive or negative status based on concordant results in at least three of the four confirmatory assays • Between 2001 and 2005, this panel was used to evaluate 19 screening assays
Confirmatory Assays • Indirect immunofluorescence IF • Western blot WB • Radioimmunoprecipitation assay RIPA • Only RIPA gave 100% agreement with the final serologic status of the specimens • Recombinant immunoblot IB • RIBA
Indirect Immunofluorescence Anti-human IgG-fluorescein conjugate Donor’s antibodies against parasite epimastigotes http://www.biologie.uni-hamburg.de/b-online/ge17/22b.jpg
http://www.molecularstation.com/images/western-blot.jpg Trypomastigote antigens Anti-human IgG conjugate The conjugate develops colour, and the results interpreted by visual inspection for bands between 130-200 kDa
RIPA • Radiolabeled antigen fragments are combined with the specimen • Specific antibodies, if present, will bind these antigen fragments • The resulting antigen-antibody complexes are precipitated and separated by electrophoresis • The pattern is detected using autoradiography (the exposure of sensitive X-ray film by the radioactive emissions of the bound, labeled antigens)
Recombinant immunoblot (RIBA) • Recombinant parasite antigens are applied to paper strips • Exposure to specimen allows anti-parasite antibodies, if present, to bind to the antigen • Anti-human labelled conjugate allows visualization
Results • 437 specimens • Positive 39% • Negative 61% • Inconclusive 2% (excluded from analysis) • Since their true serologic status cannot be determined, there is no way to conclude how they might have affected the calculated sensitivities and specificities
Results • Screening assays • Sensitivity and specificity varied considerably • Sensitivity 80%-100% • Specificity 60-100% • EIAs performed better than other screening methods • Four EIAs had specificity and sensitivity in excess of 99%
Conclusions • At least four of the commercially available EIAs are sufficiently sensitive and specific for use as a single-assay screen of blood donations • The majority of commercially available indirect hemagglutinin assays should not be used • Sensitivity and/or specificity was low • Subject to reader bias • False negatives reported even for high-titre specimesn (prozone effect) • The RIPA is the gold standard • But it is complex
Evaluation • What is the background/rationale for the investigation? • There was a clear need for establishing a Chagas panel • The report helps to raise awareness among clinicians/blood bankers about the challenges of evaluating new assays
Evaluation • Study design • The setting was a blend of the small Latin American endemic countries with the resources of WHO over several years • Variables • Variables and confounders (e.g. concurrent disease) were left undescribed • Diagnostic criteria (e.g. diagnostic test) varied from country to country
Evaluation • Bias • Bias is a possible confounder, since there was no apparent randomization in the submission of samples • Centres may have submitted specimens that were “easy” (clearly positive or negative), or specimens that were challenging • Submitting either a preponderance of easy or tough specimens could affect the sensitivity and specificity of the test results
Evaluation • Study size • No particular study size was pre-determined
Evaluation • Statistical methods were not described in detail • 95% CI were calculated and provided
Evaluation • Participants • The number of specimens received was reported • The number of specimens eventually excluded from the study also reported • Main results • Sensitivities, specificities and 95% CI were reported for the 19 screening methods and the four confirmatory assays • The “gold standard” was the consensus result of the four confirmatory assays
Evaluation • Results • Four EIA kits were appropriate to be used as single assay screens • RIPA is proposed as the gold standard • Limitations & Generalization • The specimens provided by the blood services may differ from those that would be randomly encountered (especially in countries were Chagas is not endemic) • Questions of cost and availability for small blood services • Issues of convenience with RIPA technology