Download
1 / 15
150 likes | 299 Vues
Neurofibromatosis 1 associated pain syndromes. Thomas J Geller, MD NF clinic director, CGCH Assoc Prof Neurology, SLU. Frequency of Pain as a complaint in Neurofibromatosis patients.

E N D
Neurofibromatosis 1 associated pain syndromes Thomas J Geller, MD NF clinic director, CGCH Assoc Prof Neurology, SLU
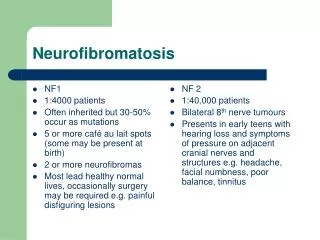
Frequency of Pain as a complaint in Neurofibromatosis patients • Though numerous neurologic complications of NF-1 appear (optic gliomas, subcutaneous neurofibromas, macrocephaly, plexiform neurofibromas, seizures, LD’s), the most common symptoms causing disability for adult patients are pain symptoms. (11.3 % in Zeller’s 1 year study of 158 adults)
Headache studies in NF-1 • North reports an incidence of 9% of severe headache. • Zeller found adult incidence of disabling headache to be 18%, but did not break out the patients with common migraine. • Recurring headache in DiMaurio’s study occurred in 46% of NF patients; 14% met criteria for migraine, 18% tension headache. • Other studies show that migraine incidence in the general population is about 18%, regardless of severity.
Quality of life with painful complications of NF-1 • French dermatology study of mixed adult/ ped NF-1 demonstrated that for all aspects of the general questionnaire, including bodily pain, pts with NF-1 reported lower QOL scores than the general population. • Increased severity of the disease was assoc with increased negative effect on bodily pain.
Pediatric NF Pain study • Oostenbrink studied 34 NF Dutch children from 1 to 6 yrs of age using the infant/toddler QOL index. • Added 7 questions on pain and limitations of activity • A significant difference in QOL was identified from kids with bodily pain vs those without bodily pain.
Non-headache pain: (bodily pain) • In the 18 adults with chronic pain, symptoms began in childhood in 7. • Pain was felt to be clearly organic in 83%. • In 17% the cause was unknown.
Causes of peripheral pain • Peripheral nerve or root- 39% • Surgical pain- 22% • Malignant peripheral nerve sheath tumor-17% • plexiform neurofibroma- 11% • Subcutaneous neurofibroma-11%
Outcome of peripheral pain in NF-1 • 77% were able to achieve at least partial remission of pain. • Pain was intermittent in ½ of patients. • Chronic pain was complicated by “breakthru” with movement or contact of the affected nerve region in most patients. • Optimal pain management was considered to be analgesics, antidepressants and/or anticonvulsants. Some required neuro-stimulation or spinal procedures.
Theoretical mechanisms of pain supersensitivity in NF-1 • Changes in the excitability of dorsal root entering the spinal cord • Study of sensory cultured neurons reveals enhanced excitability of neurons, and increased release of pain neurotransmitters CGRP and substance P. • Anxiety in the subject over the risk of pain being associated with a malignancy
Neuropathic May be caused by several processes • Direct tumor infiltration • Nerve damage / demyelination • Nerve compression • Radiation • Chemotherapy (taxols & vincristine) • Viral • Metabolic
Spontaneous burning Intermittent Radiating Shooting Light touch (allodynia) Sharp Stabbing Pins & needles Neuropathic
Cornerstones of treatment of neuropathic pain • Because neuropathic pain has both peripheral and central mechanisms of development and enhancement, treatment is probably best when multiple methods of attack are applied. • Treatment should be applied early to avoid “wind-up” mechanisms of enhanced pain
Agents for neuropathic pain • Analgesics including opioids when needed • Ketotifen for neurofibromas (esp with itching) • Calcium channel blocking anticonvulsants, (Neurontin and Lyrica) • Norepinephrine and serotonin blockers, (tricyclics and Cymbalta) • Possibly sodium channel blockers • PHYSIOTHERAPY • Relaxation therapies • Surgical management