Download
1 / 46
470 likes | 793 Vues
Interdisziplinäre Viszeralmedizin Zystische Pankreasläsionen. Endoscopic treatment of Pancreatic Necrosis and Pseudocysts. Christa Meyenberger Michael Sulz. Agenda. A cute pancreatitis Definitions of fluid collections When to intervene in necrotising pancreatitis

E N D
Interdisziplinäre Viszeralmedizin Zystische Pankreasläsionen Endoscopictreatmentof PancreaticNecrosis and Pseudocysts Christa Meyenberger Michael Sulz
Agenda • Acutepancreatitis • Definitionsof fluid collections • Whentointervene in necrotisingpancreatitis • Methodsforinterventions in WOPN • Endoscopictechniquesofdrainage/necrosectomy • Risksandcomplications in EUS-guideddrainage • Howlongstenting? • Endoscopicnecrosectomy: • Outcome data in literatureandourownexperience • Pseudocysts • Key messages
AcutePancreatitis (AP) • 85% Interstitial AP • Mortality 3% • Organ failure 10% • Recoverywithin 5-7 d • 15% Necrotising AP • Mortality 15% • Organ failure 54% • Organ failure 66% withinfectednecrosis (mortality 30%) Banks PA et al. Am J Gastroenterol2006;101:2379; TsiotosGG et al. BrJ Surg 1998;85:1650; FagenholzPJ et al. Ann Epidemiol2007;17:491; Martinez J et al. Pancreatology2006;6:206; Chauhan S et al. Am J Gastroenterol 2010;105:443.
Pancreatic fluid collections Accordingtotherevised Atlanta classification • Key points • Acute fluid collections: • Lack a well-defined wall • > 1 weekdistinction • betweenAPFC vs. ANC • Usually NO treatment Banks PA et al. Gut 2013;62:102-111.
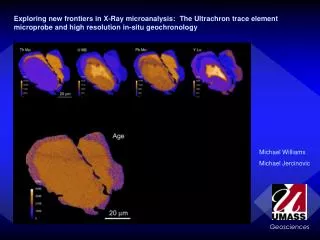
Acutenecroticcollection (ANC) Stars: necrosis; arrows: bordersofthe ANC Banks PA et al. Gut 2012;62:102-111.
Acutenecroticcollection (ANC) InfectedANC Arrow heads: gas bubbles; arrows: bordersofthe ANC Banks PA et al. Gut 2012;62:102-111.
Pancreatic fluid collections Accordingtotherevised Atlanta classification Banks PA et al. Gut 2013;62:102-111.
Pancreatic fluid collections Accordingtotherevised Atlanta classification Banks PA et al. Gut 2013;62:102-111.
Natural historyofpancreaticnecrosis is variable • May remain solid orliquefy • May remain sterile orbecomeinfected • May persistordisappearover time Banks PA et al. Gut 2013;62:102-111.
Whenisinterventionindicatedfornecrosis? It’ s all abouttiming...! WAIT at least 3-4 weeks Besselink MG et al. ArchSur 2007;142:1194-1201.
Whenisinterventionindicatedfornecrosis? Infectednecrosis (WOPN) • High suspicionfororknowninfected WOPN • Early interventionshouldbeavoidedwheneverpossible • (wait >4weeks) Symptomatic sterile necrosis (WOPN) • Intractablepain • Obstructivesymptoms (gastricoutlet/ biliaryobstruction) • Inabilitytoeat Freeman ML et al. Pancreas 2012;41:1176-1194; Baron TH et al. ClinGastroenterolHepatol 2012;10:1202-1207.
Availablemethodsforintervention in pancreaticnecrosis Endoscopic Image-guidedpercutaneous Minimally-invasive surgery Open surgicalnecrosectomy Freeman ML et al. Pancreas 2012;41:1176-1194.
Availablemethodsforintervention in pancreaticnecrosis Endoscopic Image-guidedpercutaneous Minimally-invasive surgery Open surgicalnecrosectomy Last choice! Freeman ML et al. Pancreas 2012;41:1176-1194.
Whyendoscopictreatment of WOPN? • First randomizedtrial (PENGUIN trial) comparing • endoscopicandsurgicalpancreaticnecrosectomy • Significantreductionofproinflammatoryresponse (IL-6) • Significantreductionofmajorcomplications • (20% vs. 80%; P=0.03) • Reductionofpancreaticfistula (10% vs.70%; P=0.02) Endoscopicnecrosectomyhasthe potential for a quantumleaptoimproveoutcome in WOPN Bakker OJ et al. JAMA 2012,307:1053-1061.
Endoscopictechniquesofdrainage/necrosectomy • Peroral flexible endoscopicdrainage • transpapillarytransmural • Directendoscopicnecrosectomy • Nasocysticcatheter Freeman ML et al. Pancreas 2012;41:1176-1194.
EUS-guided drainage of pancreatic collections Whatyouneed Conscioussedation 2. EUS linear scope, operating channel >3.6mm 3. 19-gauge needle 4. Two 0.035 inch (0.89 mm) guidewires(superstiff) 5. Cystotome10 Fr Two double pigtailstents (7 F, 5 or 7 cm) Nasocysticcatheter(6 F) Barthet M Gastroenterol Clin Biol 2008;32:128-33; Barthet GIE 2008;67:245-52; Seewald S Endoscopy 2009;41:166-174.
EUS-guided drainage of pancreatic collections Visualisation • Significantlyhighertechnicalsuccessthanwithout EUS • (100 vs. 33%, P<0.001)1 Exclude interposedvessels using Doppler ultrasound 1 Vadararajulu S et al. GIE 2008;68:1102-1111. Park DH, Endoscopy 2009 (PRC; n= 60)
EUS-guided drainage of pancreatic collections Puncture & guidewireinsertion 2 loops
EUS-guided drainage of pancreatic collections Ballon dilatation & secondguidewire
EUS-guided drainage of pancreatic collections Insertion ofpigtail & nasocysticcatheter 7 F nasocysticcatheter 10 F double pigtail Irrigation with 1500 ml saline/24h via nasocysticcatheter
Endoscopic necrosectomy ( Dilateupto 18-20 mm Insert a therapeuticgastroscope, generouslavage, Remove debris • Instruments: • Dormiabasket • Retrievalnets • Soft snares Nasocysticcatheter
EUS-guided drainage: Be aware of… Perforation Distanceto GI-wall
Risks of EUS-guided drainage: Perforation • Relative risk : 0.9 to 3 % • Related to the distance between the digestive wall / cyst lumen: • usually< 1 cm • in fact possible up to 2 cm Use CO2 insufflator Barthet M et al. Gastroenterol Clin Biol 2008;32:128-33; Barthet M et al. GIE 2008;67:245-52; SeewaldS et al. Dig Endosc2009;21:S61-5; Giovannini et al. GI Clin N Am 2012;22:221-30.
EUS-guided drainage: Be aware of… Perforation Distanceto GI-wall Interposedvessels Bleeding
Risks of EUS-guided drainage: Bleeding • Rate: 1 - 6 % • Immediate: • Due toportalhypertension • Due tointerposedvessels • Delayed: • Dueto erosion of vessels inside the PC wall (pseudoaneurysma) • Management by interventional coiling orEUS-guidedembolization Use EUS and/or CECT Barthet M et al. Gastroenterol Clin Biol 2008;32:128-33; Barthet M et al. GIE 2008;67:245-52; SeewaldS et al. Dig Endosc2009;21:S61-5; Giovannini et al. GI Clin N Am 2012;22:221-30.
EUS-guided drainage: Be aware of… Perforation Distanceto GI-wall InInterposedvessels Bleeding Infection Presence ofdebris, Diameter ofcollection
EUS-guided drainage: Be aware of… Perforation Distanceto GI-wall InInterposedvessels Bleeding Infection Presence ofdebris, Diameter ofcollection Migration/ Recurrence Typesofstents (Pigtail/Metal)
Risks of EUS-guided drainage: Stent migration • Rate: <1 % • Immediate migration: • Technical problems with release • Double pigtail (marker!) • Metal stent (inside release) • Delayed migration: metal stent Barthet M et al. Gastroenterol Clin Biol 2008;32:128-33; Barthet M et al. GIE 2008;67:245-52; SeewaldS et al. Dig Endosc2009;21:S61-5; Giovannini et al. GI Clin N Am 2012;22:221-30.
Risks of EUS-guided drainage: Recurrence • Rate: 5-10 % • Early stent removal = Risk of recurrence • MRI assessment of the main pancreatic duct • Duct leakage: transpapillary pancreatic duct stenting to maintain integrity • Disconnected duct syndrome: Leave pigtails indefinitely in place • Role of stent type • At least two double pigtail (7 F sufficient!) • Metal stent ? Barthet M et al. Gastroenterol Clin Biol 2008;32:128-33; Barthet M et al. GIE 2008;67:245-52; SeewaldS et al. Dig Endosc2009;21:S61-5; Giovannini et al. GI Clin N Am 2012;22:221-30. Arvanitakis et al. GIE 2007
EUS-guided drainage: Be aware of… Perforation Distanceto GI-wall Interposedvessels Bleeding Infection Presence ofdebris, Diameter ofcollection Migration/ Recurrence Typesofstents (Pigtail/Metal)
Endoscopic necrosectomy: Outcome1 • Systematicreview (pooledanalysis) • 10 studies (260 patients; 60% proventobeculture-positive necrosis) • 1996-2009 • Systematicreview (pooledanalysis): 14 studies(455 patients; 2005-2013) • Onlyoneprospectiverandomizedstudy 1 Haghshenasskashani A et al. SurgEndosc 2011;25:3724-3730.; van Brunschof S et al. SurgEndosc 2014
Endoscopic necrosectomy: Outcome1 Endoscopic necrosectomy is safe and effective in management of WOPN 1 Haghshenasskashani A et al. SurgEndosc 2011;25:3724-3730.; van Brunschof S et al. SurgEndosc 2014
Ourown single-center experienceregarding WOPN treatment (retrospective, 2002-2013, 2 operators) Christa Meyenberger & Michael Sulz; unpublisheddata
Ourown single-center experience Christa Meyenberger & Michael Sulz; unpublisheddata
Ourown single-center experience Christa Meyenberger & Michael Sulz; unpublisheddata
Ourown single-center experience Christa Meyenberger & Michael Sulz; unpublisheddata
Ourown single-center experience Long-term qualityoflife (SF-36 score) Christa Meyenberger & Michael Sulz; unpublisheddata
Pseudocyst: • Indicationfortreatment: • Symptoms: impairedfoodintake, pain • Complications: infection, bleeding • Endoscopictreatment: • EUS-guidedtransmuralendoscopicdrainage • transgastric, -duodenal • - Transpapillarydrainge, stenting • Surgicaltreatment • Cystoenterostomy • Cystogastrostomy • Morbidity 25%, mortality 5% • Percutaneousdrainage • - Complication: fistula Köhler H, Schafmayer A, Lüdtke FE, et al. Surgicaltreatmentofpancreaticpseudocysts. Br J Surg 1987; 74:813. Gumaste VV, Pitchumoni CS. Pancreaticpseudocyst. Gastroenterologist 1996; 4:33.
Pseudocyst – Surgery versus endoscopy Onerandomizedstudy Endoscopictreatment = firstchoiceoftreatment • MRI assessment of the main pancreatic duct • Duct leakage: transpapillary pancreatic duct stenting to maintain integrity • Disconnected duct syndrome: Leave pigtails indefinitely in place or surgery Varadarajulu S, Bang JY, Sutton BS, Trevino JM, Christein JD, Wilcox CM. EqualEfficacyofEndoscopicandSurgicalCystogastrostomyforPancreaticPseudocyst Drainage in a RandomizedTrial Gastroenterology. 2013 Sep;145(3):583-90
Key messages • Definethepancreaticfluid collection(Revised Atlanta classification) • Acute fluid collection: Usuallynotreatment • Collections > 4 weeks: Distinctbetweenpseudocyst / WOPN • WOPN with solid material • Intervention in WOPN: Timing! Wait >3-4 weeks • Endoscopicinterventionsin WOPN: effectiveandsafe • Importantissues: • Distanceto GI-wall < 1-2 cm • Use EUS (interposedvessels) • MRI assessmentofmainpancreaticduct • Pseudocysts: • Endoscopictreatmentisfirstchoiceoftreatment • MRI assessmentofmainpancreaticduct
Novel multiple transluminal gateway technique for EUS-guided drainage of WOPN1 1 Varadarajulu S et al. GIE 2011;74:74-80; Figurefrom: Baron TH et al. ClinGastroenterolHepatol 2012;10:1202-1207.
Who should not perform endotherapy in WOPN? • The time challenged with full endoscopy program • Endoscopistswithout EUS access • Endoscopistswithout expert surgical and interventional • radiologic support to treat complications ... in otherwords... Who should perform endotherapy in WOPN? • Only expert pancreaticobiliaryendoscopists with special committment • Those with clinical judgementregarding the appropriate indication Baron TH et al. ClinGastroenterolHepatol 2012;10:1202-1207; Kozarek RA, GIE 2005;62:101-104.
Entscheidung zur Operation • Kriterien: • Grösse des Abszesses • Pankreasgangruptur mit fehlender • transpapillärer Ableitung • Zystojejunostomie am 10.3.2009 • Postoperativ guter AZ
Therapieempfehlung Pankreasabszess I • Interdisziplinärer Approach • Initial endoskopische Therapie, immer wenn: • Zugang endoskopisch möglich • Interventionalist mit entsprechender Erfahrung verfügbar • Ziele der endoskopischen Therapie: • Stabilisierung der Situation durch Drainage • Verhinderung von Komplikationen einer notfallmässigen Operation Seewald S et al. Aggressive endoscopictherapyforpancreaticnecrosisandpancreatisabscess: a newsafeandeffectivetreatmentalgorithm. Gastro Endosc 2005; 62: 92-100.
Therapieempfehlung Pankreasabszess II • Indikationen zur Chirurgie: • „Endoscopic failure“ • Unzureichende Entfernung von nekrotischem Material aufgrund schlechtem endoskop. Zugang • Zugang unmöglich, z.B. paracolic gutters • „Disconnected-duct syndrome“ (totale Pankreasgangruptur) • Grösse der Kollektion > 15 cm* • Ergebnisse der endoskopischen Therapie • 2/3 Kurativ • 1/3 Klinische Verbesserung mit elektiver OP im Verlauf Seewald S et al. Aggressive endoscopictherapyforpancreaticnecrosisandpancreatisabscess: a newsafeandeffectivetreatmentalgorithm. Gastro Endosc 2005;62: 92-100. * Papachristou GI et al. AnnalsofSurgery 2007;245:950.