Comprehensive Overview of Cardiac Surgical Procedures and Nursing Implications
1.02k likes | 1.3k Vues
This document outlines the essential information regarding major cardiac surgical procedures, including Coronary Artery Bypass Grafting (CABG) and other interventions such as valve replacement and aneurysm repair. Key topics discussed include indications and contraindications for surgery, physiological effects, and detailed management strategies for preoperative, intraoperative, and postoperative care in nursing. It also highlights potential complications and nursing interventions to mitigate risks. This guide serves as a valuable resource for nursing professionals involved in cardiac surgical care.

Comprehensive Overview of Cardiac Surgical Procedures and Nursing Implications
E N D
Presentation Transcript
Cardiac Surgical Procedures Nursing 409 Fall 2016-2017
Class General Objectives • Discuss and describe selected cardiac surgical procedures (PTCA-CABG) in regards to their: • Indications, contraindications, and physiological effects. • Pre, intra, and post procedure management (nursing & collaborative). • Possible complications and nursing interventions to prevent possible complications.
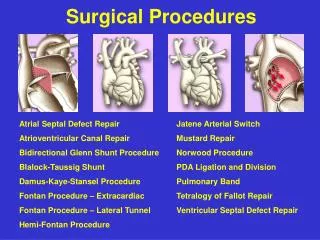
What is Open Heart Surgery? It isn’t just CABG • Valve replacement • VSD • Ascending Thoracic Aneurysm Repair • Left Ventricular aneurysm repair • Surgery to relieve hypertrophy in CMPs • All need to be on the Cardio-pulmonary pump in the OR
WHAT IS CABG • Coronary artery bypass graft is the surgical technique which uses saphenous leg veins as grafts (SVG) or the internal mammary (LIMA or RIMA) gastroepiploic/radial arteries as grafts to bypass obstructed portions of a coronary artery
WHAT IS CABG Standard surgical coronary revascularisation Requires : • CPB • Aortic cross clamping • Global cardioplegia arrest
History • 1967 the first CABAG surgery in the USA. • First open-heart surgery procedure in Jordan in 1970. • First heart-valve replacement in the country in 1972. • First coronary artery bypass in Jordan in 1973.
Indication • The 2004 ACC/ AHA CABG guidelines state CABG is the preferred treatment for: • Disease of the Left Main Coronary Artery • Disease of all three coronary vessels (LAD, LCX, & RCA). • Diffuse disease not amendable to treatment with a PTCA.
WHO NEEDS CABG?? CONDITIONS THAT NEED CORONARY REVASCULARIZATION: • Stable angina but meds not controlling pain, pt has function • Non-successful PTCA with evolving MI • Unstable angina • A positive exercise tolerance test [treadmill], & lesions or blockage that cannot be treated by PTCA • Exercise induced ventricular arrhythmias due to myocardial ischemia • A Left Main Coronary lesion or blockage of more than 60% (50%) • Single or double vessel disease with type B or C lesions
WHO NEEDS CABG?? CONDITIONS THAT NEED CORONARY REVASCULARIZATION: • Three vessel CAD (70% stenosis) with depressed left ventricular function or two vessel CAD with proximal LAD involvement. In randomized trials, patients with three vessel and depressed LV function showed survival benefit with CABG compared to medical tx. Operative mortality increases when EF is less than 30%. • Other: post infarct angina, thrombosis after PTCA
AHA/AC AHA/ACC Definition of Classes for Various Conditions C Definition of C AHA/ACC Definition of Classes for Various Conditions • Class I--Conditions for which there is evidence and/or general agreement that a given procedure or treatment is useful and effective. • Class II--Conditions for which there is conflicting evidence and/or a divergence of opinion about the usefulness or efficacy of a procedure. • Class IIa--The weight of evidence/opinion is in favor of usefulness/efficacy. • Class IIb--Usefulness/efficacy is less well established by evidence/opinion. • Class III--Conditions for which there is evidence and/or general agreement that the procedure/treatment is not useful/effective and, in some cases, may be harmful.
ACC/AHA Guidelines for Coronary Artery Bypass Graft Surgery In Asymptomatic or Mild Angina Class I 1. Significant left main coronary artery stenosis. 2. Left main equivalent: significant ( 70%) stenosis of the proximal LAD and proximal left circumflex artery. 3. Three-vessel disease. (Survival benefit is greater in patients with abnormal LV function; e.g., EF <0.50.) Class IIa Proximal LAD stenosis with 1- or 2-vessel disease.* Class IIb One- or 2-vessel disease not involving the proximal LAD.
CABG indication for other Class I conditions Stable Angina 1. Significant left main coronary artery stenosis. 2. Left main equivalent: significant ( 70%) stenosis of the proximal LAD and proximal left circumflex artery. 3. Three-vessel disease. (Survival benefit is greater when LVEF <0.50.) 4. Two-vessel disease with significant proximal LAD stenosis and either EF <0.50 or demonstrable ischemia on noninvasive testing. 5. One- or 2-vessel CAD without significant proximal LAD stenosis, but with a large area of viable myocardium and high-risk criteria on noninvasive testing. 6. Disabling angina despite maximal noninvasive therapy, when surgery can be performed with acceptable risk. If angina is not typical, objective evidence of ischemia should be obtained.
CABG indication for other Class I conditions Unstable Angina/Non-Q Wave MI 1. Significant left main coronary artery stenosis. 2. Left main equivalent: significant ( 70%) stenosis of the proximal LAD and proximal left circumflex artery. 3. Ongoing ischemia not responsive to maximal nonsurgical therapy. ST-Segment Elevation (Q-Wave) MI None. Poor LV Function 1. Significant left main coronary artery stenosis. 2. Left main equivalent: significant ( 70%) stenosis of the proximal LAD and proximal left circumflex artery. 3. Proximal LAD stenosis with 2- or 3-vessel disease.
CABG indication for other Class I conditions Life-Threatening Ventricular Arrhythmias • Left main coronary artery stenosis. • Three-vessel coronary disease. After Failed PTCA • Ongoing ischemia or threatened occlusion with significant myocardium at risk. • Hemodynamic compromise. With Previous CABG Disabling angina despite maximal noninvasive therapy. (If angina is not typical, then objective evidence of ischemia should be obtained.)
EMERGENCY VS ELECTIVE CABG • The outcomes of the CABG are very dependent on the pre-op conditions!! • Emergency cases come from the cath lab with death of tissue & many anticoagulants on board • Elective cases come from home NPO & prepared
CABG Versus Balloon Angioplasty A systematic review of the 22 RCTs comparing CABG with balloon angioplasty concluded the following : • Survival was similar for CABG and PCI (with balloon angioplasty) at 1 year and 5 years. • Survival was similar for CABG and PCI in subjects with 1-vessel CAD (including those with disease of the proximal portion of the LAD artery) or multivessel CAD. • Incidence of MI was similar at 5 years after randomization.
CABG Versus Balloon Angioplasty • Procedural stroke occurred more commonly with CABG than with PCI (1.2% versus 0.6%). • Relief of angina was accomplished more effectively with CABG than with PCI 1 year after randomization and 5 years after randomization. • During the first year after randomization, repeat coronary revascularization was performed less often after CABG than after PCI (3.8% versus 26.5%).
Characteristics of Graft • Diameter similar to coronary arteries. • No disease or vessel wall abnormalities. • Adequate length. • Commonly used grafts: • Saphenous vein graft • Internal mammary artery grafts
Saphenous Vein Graft • Anastomoses one end of vein to aorta (proximal) and other end to coronary artery past obstruction (distal) • May be simple or sequential (also called skip) • May be taken from above or below the knee • About 50% occluded after 10 years • Vein failure: • Thrombosis • Fibrointimal hyperplasia • Atherosclerosis
Vessel Patency 1. internal mammary artery graft 90% patency at 10 years 2. saphenous vein graft 50% patency at 10 years 3. PTCA of stenotic vessel 60% patency at 6 months 4. PTCA + stent of stenotic vessel 80% patency at 6 months
LIMA is the most commonly usedArterial graft, most often used as aPedicle graft, most commonly grafted W/ LAD, 90-95% 10 yr patency 10 yr patency for vein grafts is 50%
Internal Mammary Artery Grafts • Preferred alternative to saphenous • Used as a pedicle graft to bypass diseased artery • Both left and right can be used. • Left internal mammary artery longer and larger • Used to bypass LAD • Right internal mammary artery is used for right coronary artery or LCX. • 90% patency at 10 years
Other Grafts • Radial artery • More prone to spasm • Postoperative add nitroglycerin followed by oral nitrates • Right gastroepiploic artery • Homologous (nonnative) grafts • Saphenous, umbilical, or bovine internal mammary artery
Factors associated with bypass surgery • Age. • pervious heart surgery. • Lt V EF. • percentage of stenosis. • number of coronary blood vessels that need grafting. • Gender. • Having another serious medical condition such as diabetes, peripheral vascular disease, kidney disease or lung disease • Current Hemodynamic status • Concurrent medical conditions especially DM & COPD
Cardiopulmonary Bypass • Moves oxygenated blood around the body during open heart surgery • Core body temp is lowered to 28° C to 32° C • Complications • Increased capillary permeability • Hemodilution • Altered coagulation • Damage to blood cells • Microembolization
Cardiopulmonary Bypass Complications • Arrhythmias • Fluid resuscitation • Decreased cardiac contractility • Control of blood pressure • Respiratory problems • Postoperative bleeding
Overview of CABG procedure Expose breast bone Skin incision Divide breast bone Retractor placed
Overview of CABG procedure pericardiotomy Heart visualized Aortic cannula brings blood from CPB to aorta Venous cannula drains blood From heart to CPB
Overview of CABG procedure Cardioplegia tube In coronary sinus Cardioplegia tube inserted In aorta
Overview of CABG procedure Heart stopped, aortic clamp Placed, no flow in heart Bypass vessel grafted Clamp removed, Cardioplegia reversed Heart beating normally, CPB stopped
Overview of CABG procedure Sternum closed w/ Metal wire Chest tubes placed Sterile bandage applied Skin closed
Newer Techniques • Off-pump CABG surgery (OPCABG) • Decreased length of stay • Incidence of stroke 48 to 72 hours (vs. immediately after surgery if on cardiopulmonary bypass) • Minimally invasive direct coronary artery bypass grafting (MIDCABG) • Number of grafts restricted
Transmyocardial Laser Revascularization (TMLR) • Option for unstable angina refractory to interventions • Eligibility: • Prior CABG surgery, multiple cardiac interventions with maximal medication • Physiology of laser • Angiogenesis • Direct channel patency
Post-TMLR Care • Inotropic support • Monitoring fluid status • Antiarrhythmic therapy • Manage angina. • Monitor ST segment. • Anticoagulation therapy
Cardiac Surgery • Preoperative care • Typical preparation
Preoperative Phase • Patient and family need special preparation to decrease level of anxiety • Educational preparations • Tour of the ICU waiting room, intermediate care unit • Have the patient talk and communicate with other patients recovering from the same surgery • Expectation before the surgery: • Diagnostic test • Skin preparation • NPO at least 8 hrs • Deep breath & coughing exercise, leg exercises • Expectation during the surgery • Expected time of the surgery • Type of the procedure • Family waiting room
Preoperative Phase • Expectation after the surgery: • Name and location of the ICU • External devices such as ventilator, NGT, ECG electrodes, central lines, chest tubes, & foley catheter • Expected procedures such as endotracheal suctioning, blood administration, activity progression • Expected ICU noise & family involvement • Additional preparations include • Results of preoperative laboratory test should be within normal range (e.g., blood chemistry, CBC, PT, PTT, ECG, chest x-ray, blood type) • Shower with antibacterial soap • Essential medication may be given early morning
PRE-OP NURSING CARE • Teaching: • what this procedure will do for the patient’s pathology- it is not a cure • cough, deep breath, splint incision • what the all the tubes do: chest, swan, Foley, ET, leads • wound care- legs and sternum, possible complications of osteomyelitis of the sternum • Meds: effects of Nitro, dopamine, dobutamine & pain meds • Anticipate mood changes or depression, anxiety, & forgetfulness *new push to do CABG off the pump • Pre-op risk factor modification • Need for continuation of cardiotonic meds to prevent ischemia prior CABG • Re-hydration may be necessary, if on chronic diuretics
TEACHING NEEDS OF THE “REDO” • It is a common misconception that patients who have already had CABG and need a “redo” do not need pre-op education- “they already know what will come.” • Recent nursing research shows these patients have the same learning needs as the first timers. These same patients had a special interest in knowing who the health care workers were & what they would be doing for the patient