CLINICAL CASE
IRON DEFICIENCY ANEMIA AND ANCYLOSTOMA DUODENALE Onofre Alarcón, Antonio Sánchez del Río, Salvador Baudet, Servicio de Digestivo. Tenerife. Canary Islands. Spain . INTERNATIONAL COURSE ON CAPSULE ENDOSCOPY ICCE 2005 Miami Florida USA. CLINICAL CASE


CLINICAL CASE
E N D
Presentation Transcript
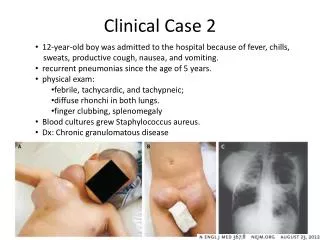
IRON DEFICIENCY ANEMIA AND ANCYLOSTOMA DUODENALEOnofre Alarcón, Antonio Sánchez del Río, Salvador Baudet, Servicio de Digestivo. Tenerife. Canary Islands. Spain INTERNATIONAL COURSE ON CAPSULE ENDOSCOPY ICCE 2005 Miami Florida USA CLINICAL CASE A 58 year old man with iron deficiency anemia was referred to our Unit for a wireless capsule endoscopy Study. He had no diarrhea, abdominal pain, weight loss or rectal bleeding. A hemoccult test was positive, so he had been previously studied with a full colonosocpy, upper endoscopy and small bowel series with negative resultaste patient had no family history of cancer or inflammatory bowel Disease. He had not past history of peptic disease, NSAIDs intake or alcohol consuption. Celiac disease was also ruled out and a hematologic consultation show not any other specific consultation. A wireless capsule endoscopy study was done, showing multiple round small ulcers, some fresh and some covered with black fibrina, along the distal jejunum and ileum. At ileum several white, small filliform figures attached to the bowel wall were found. They showed a slightly dilatated reddish portion in the anchorage point. A suspicion diagnosis of hookworm disease was done, confirmed with a direct fecal examination which showed oval eggs . Treatment with iron repletion and antihelmintic therapy with albendazole was started, and the anemia resolves DISCUSSION Hookworm infection is a worlwide intestinal parasitic disease afeccting more than one billion people. It is caused by the nematodes Ancylostoma duodenale, Necator americanus and Ancylostoma ceylonicum. A duodenale and N americanus are white, cylindrical worms 0.8-1.5 cm long. Ancylostoma duodenale (Old World hookworm) is found in most areas of the World , especially Asia, Africa, Middle East and Southern Europe. In North and South America predominates Necator americanus (New World hookworm). Adult hookworms anchor themselves in the mucosa of the small intestine. The teeth of the adult hookworm allow it to grip the intestinal mucosa. The worm secretes an anticoagulant that facilitates the ingestion of blood and juices from its host. They periodically change their location, which can explain the multiple, different stage ulcers we found in the capsule exam. Although hookworm infection represents an important public health problem in developing countries the immigration process to Western countries has increased the recognition of this disease as a cause of anemia. Diagnosis of hookworm is usually based on finding the characteristic eggs in the stool. The clinical manifestations of hookworm infection depends on the life cycle of the organism and the intensity of infection. The symptoms include skin irritation, pruritus, cough, wheezing, epigastric pain or abdominal tenderness. However the hallmark of chronic hookworm disease is iron deficiency anemia, as was the case of our patient. Fresh ulcer Fresh ulcer Ulcer with clot A duodenale A duodenale A duodenale and ulcer • CONCLUSIONS • Hookworm infection represents an important public health problem in developing countries. • The inmigration process to Western countries has increased the recognition of this disease as a cause of anemia. • As wireless capsule endoscopy has become the procedure of choice for small bowel imaging in the evaluation of iron deficiency anemia physicians performing this test must be familiarized with the capsule findings of hookworm infection. BIBLIOGRAPHY Pearson RD Parasitic diseases: helminths Chapter 109, 2442-2459 In Tadataka Yamada Textbook of Gastroenterology volume 2 Third edition Lippincott Williams & Wilkins Philadelphia 1999 Roca C, Balanzo X, Sauca G, Fernandez-Roure JL, Boixeda R, Ballester M Imported hookworm infection in African immigrants in Spain A study of 285 patients Med Clin (Barc) 2003 Jun 28; 121(4):139-41