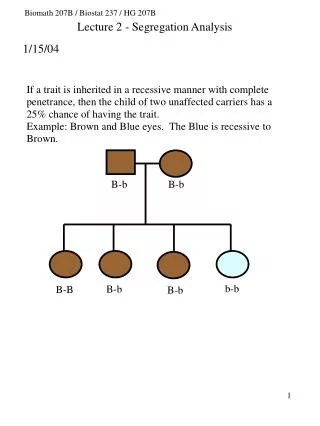
B B
P P. B B. Dornhorst: Lancet 1955. Hogg J et al. NEJM 2004. Hogg J et al. NEJM 2004. Flow-Volume Curve. Normal. Severe-obstruction. From Pride N. in Calverley PMA: COPD, 1995. ROCA J. 2002. Emphysema by CT scan.

B B
E N D
Presentation Transcript
P P B B Dornhorst: Lancet 1955
Flow-Volume Curve Normal Severe-obstruction From Pride N. in Calverley PMA: COPD, 1995
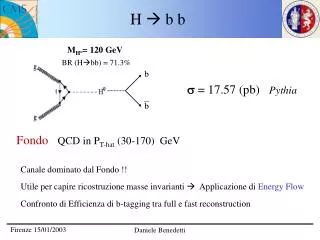
Emphysema by CT scan Poor correlation with mild anatomical emphysema. Moderate correlation with function Does not detect PLE of degrees as high as 30/100. Emphysema can be present with normal function.
FEV1/FVC = ridotto FVC = ridotto L’IMPORTANZA DI MISURARE TLC Ostruzione oppure Ostruzione e restrizione?
OBSTRUCTION (PSEUDORESTRICTION) RESTRICTION FEV1/FVC = normale FVC = ridotto L’IMPORTANZA DI MISURARE TLC Ostruzione o Restrizione ?
ALTRI ACCERTAMENTI (4) a cura dello pneumologo ANOMALIA OSTRUTTIVA? ANOMALIA OSTRUTTIVA? PERSONA A RISCHIO (2) STOP SINTOMI RESPIRATORI? (1) SI’ NO NO SPIROMETRIA GLOBALE + TEST DI BRONCODILATAZIONE + EVENTUALE VISITA PNEUMOLOGICA (3) NO SI’ SI’ SI’ DIAGNOSI DI BPCO SPIROMETRIA SEMPLICE + TEST DI BRONCODILATAZIONE + EVENTUALE VISITA PNEUMOLOGICA (3) NO FOLLOW UP STADIAZIONE E TRATTAMENTO a cura dello pneumologo • Ricerca attiva dei sintomi, anche con questionari ad hoc, ogni 1-2 anni, se presente rischio • Utilizzo carte del rischio CNR-ISS • Spirometria semplice • Per altre malattie respiratorie o di altri apparati. MMG PERCORSO DIAGNOSTICO DELLA BPCO
“IF PULMONARY FELLOWS BEGINNING THEI TRAINING FULLY UNDERSTOOD ALL THE MATERIAL ON GAS EXCHANGE AND MECHANICS, THE WORLD WOULD BE A BETTER PLACE”. • John West. Respiratory Physiology. The Essential. 2005
Lung volumes during exercise: dynamic hyperinflation in COPD IRV = inspiratory reserve volume
FVC FEV1<65%pr Testo
Rate of moderate and severe exacerbations over three years Mean number of exacerbations/year 25% reduction 1.2 1.13 0.97* 0.93* 1 0.85*†‡ 0.8 0.6 0.4 0.2 0 Placebo SALM FP SALM/FP Treatment *p < 0.001 vs placebo; †p = 0.002 vs SALM; ‡p = 0.024 vs FP
NOTA EMA-AIFA • Per salmeterolo50/Fluticasone500 mcg bid “trattamento sintomatico di pazienti con BPCO, con FEV1<60% del predetto pre-broncodilatatore ed una storia di riacutizzazioni ripetute, che abbiano sintomi significativi nonostante la terapia regolare con broncodilatatori”. 50