Download
1 / 32
370 likes | 974 Vues
STROKE ACUTE CARE and THROMBOLYSIS Adrian Pace Neurology SpR Derriford Hospital. Types of Stroke. Stroke is several different disease processes: Small vessel disease (atherosclerosis) Large vessel disease (carotid atheroma embolism) Cardio-embolic disease (AF; PFOs; LVF)

E N D
STROKE ACUTE CARE and THROMBOLYSIS Adrian Pace Neurology SpR Derriford Hospital
Types of Stroke Stroke is several different disease processes: Small vessel disease (atherosclerosis) Large vessel disease (carotid atheroma embolism) Cardio-embolic disease (AF; PFOs; LVF) Cerebral haemorrhage (aneurysms; HTN)
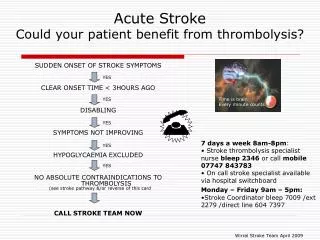
Acute care in a nutshell Oxygen, glucose, blood pressure Sa02 should be maintained at >=95% Blood glucose should be maintained between 4 – 11 mmol including use of insulin for known diabetics Blood pressure should allowed to find its normal level by ensuring normal fluid balance
Also in first 24 hours… • Admit to an acute stroke unit direct from ED • Aspirin 300 mg • Swallow screen and SALT referral • Keep temperature down (fan, paracetamol) • Early mobilisation and PT referral • Avoid catheters unless in retention
National guidelines • Everything you need is in the • Royal College of Physicians National Clinical Guidelines for Stroke (3rd Edition) 2008 • This includes a comprehensive evidence-based guide to acute stroke care – what works, what is pointless, what is still being tested
THROMBOLYSIS FOR ISCHAEMIC STROKE
Ischaemic cascade in stroke Process of stroke injury at cellular level. Irreversible damage begins immediately at the core (Umbra). The surrounding area (Penumbra) is an ischaemic zone with CBF of 25-50% of normal and loss of autoregulation. Viability of penumbra is preserved if perfusion is restored with in a critical time period.
Ischaemic Penumbra Maintain blood flow to penumbra Maintain cerebral blood flow
Thrombolysis is the process of breaking up and dissolving intravascular blood clots by pharmacological means. • Some commonly used thrombolytics are: • Streptokinase • Urokinase • Recombinant tissure plasminogen activators (rt-PA). • Thrombolysis is used for minimising tissue damage following myocardial infarction, stroke, massive pulmonary embolism and acute limb ischaemia. Thrombolysis reduces risk of long term disability after stroke by 30% But only 0.2% received thrombolysis in UK in 2006 compared with 10% in Australia. Derriford currently at about 1.5% of acute stroke admissions. NAO estimate: - cost of thrombolysis for 9% strokes to be £9.9 million - saving of £26.4 million in care costs
Benefit vs Harm with Thrombolysis For every 100 patients treated with rt-PA: - 32 have a better final outcome - 3 have a worse final outcome - 65 have an unchanged outcome NNT = 3.1 NNH = 30.1 Likelihood of being helped rather than harmed LHH = 30/3 = 10 Intravenous rt-PA is 10 times more likely to help than harm eligible patients with acute ischaemic stroke.
Risk of Cerebral Haemorrhage with rt-PA 6.4% risk of symptomatic ICH within 24hrs (ie, clinical worsening due to new ICH) vs 0.6% without rt-PA. 1.5% risk of large haemorrhage with significant space occupying effect likely to prove fatal and not usually amenable to surgery. At three months mortality was not significantly different between the two groups
ELIGIBILITY FOR THROMBOLYSIS
Eligibility Criteria for treatment with rt-PA • Age 18 to 80 years • Clinical diagnosis of ischaemic stroke • Stroke must cause a measureable • neurological deficit (NIHSS >4) • Time of symptom onset is known • Sufficient time in 3 hours therapeutic • window to assess and treat • No clear contraindication to • thrombolysis.
Contraindications to Thrombolysis (1) • HISTORY • Haemorrhagic retinopathy • Known or suspected history of intracranial bleed • HI or stroke within last 3/12 • Major surgery/trauma within last 3/12 • Peptic ulcer • Recent puncture of a non-compressible blood vessel • Recent (<10/7) traumatic CPR or childbirth • Severe liver disease • Neoplasm with increased bleeding risk • Prior stroke with concomitant diabetes
Contraindications to Thrombolysis (2) • CURRENT • Symmptoms suggestive of SAH • Evidence of intracranial bleed on CT • Seizure at onset of stroke • SBP of >185mmHg or DBP >110mmHg • Symptoms rapidly improving before rt-PA • Anticoagulants (except warfarin if INR <1.4) • Platelet count below 100x103 • Clinically mild stroke (NIHSS <4) • Clinically severe stroke (NIHSS >25) • Severe stroke as assessed on CT (>1/3 MCA territory;) • Previous functional status (Rankin score 3 or more)
ACUTE MANAGEMENT IN HOSPITAL
NINDS recommended targets for time • Door to Doctor 10 minutes • Access to Neurological expertise 15 minutes • Door to CT completion 25 minutes • Door to CT interpretation 45 minutes • Door to treatment 60 minutes • Admission to monitored bed 3 hours
Acute Management Vitals: A : Is the airway secure? B : O2 saturation > 95%? (put all patients on an oxygen mask) C : BP? Too high or too low? Is patient in AF? History: - Symptom onset or time last seen normal - Correlate times (alarms, work, drive time TV) - Corroborate with any available witness - Prodromal or previous symptoms/TIAs - Exclude stroke mimics ***IS THE PATIENT A CANDIDATE FOR THROMBOLYSIS?***
Thrombolysis in the ED • IDENTIFY POTENTIAL CANDIDATE • IMMEDIATELY CONTACT STROKE PHYSICIAN • Take bloods (FBC, U&Es, glucose, clotting) • Acquire a 12-lead ECG • IV access x 2 (preferably large gauge) • Document observations every 15 minutes • Check capillary BM • Administer O2 at 2-10 L/min • If BP consistently >185 SBP or >110 DBP - labetolol • ORGANISE IMMEDIATE CT SCAN
Stroke Physician Assessment • Examine patient and confirm diagnosis • Discuss risks/benefits with patient/relatives • Obtain informed consent • Review and confirm inclusion/exclusion criteria • Complete NIHSS and Rankin scores • Obtain weight estimate • Review blood results and CT images • Calculate dose of rt-PA • - 0.9 mg/kg (max. 90mg) • - 10% dose stat over 1 min • - remaining 90% over 1 hour • Patient admitted to Level 1 area
POST-THROMBOLYSIS ASSESSMENT AND MONITORING
Post Thrombolysis (1): The ‘DOs’ • Check observations: • - every 15 minutes for 2 hours • - every 30 minutes for 6 hours • - every 60 minutes for 16 hours • NIHSS at 2 hrs, 24 hrs and 7 days ( or discharge) • Maintain oxygenation • Treat pyrexia aggressively • Manage blood glucose actively • Prompt swallowing assessment • IV fluids if needed • Nurse with head and trunk at 30 degrees in bed
Post Thrombolysis (2): The ‘DON’Ts’ • For the first 24 hours (unless absolutely necessary): • No urinary catheters • No NG tubes • No aspirin / dipyridamole / clopidogrel • No heparin (not even prophylactic doses • Avoid central venous and arterial lines
24 hours Post-Treatment Likelihood of rt-PA complications reduced Usual stroke aftercare resumes: 1. aspirin 300mg after repeat scan 2. NG tube if required 3. Investigations of stroke aetiology as indicated 4. Secondary prevention therapy 5.Begin normal rehabilitation
BP Management Post-Thrombolysis • Significant HTN post-treatment is potentially hazardous due to haemorrhagic transformation. • SBP >180 or DBP >105 on two occasions over 5 minutes: • Labetolol 10-20mg IV stat • Repeated dose Labetolol can be used • Consider Labetolol infusion • GTN infusion (as per cardiac dosing) • Avoid Ca+ channel blockers • Na+ nitroprusside infusion on ITU
Neurological Deterioration Post Thrombolysis ICH may be signalled by acute HTN, headache, neurological deterioration, and N&V. Inform Stroke team immediately Repeat CT head Contact neurosurgeons if haemorrhage - stop rt-PA infusion! - check FBC and clotting - Give FFP, cryoprecipitate, platelets Treatment is usually conservative
BARRIERS TO RAPID ACUTE STROKE CARE
Patient inability to recognise stroke symptoms • - 40% of stroke patients cannot name a single sign or symptom or • stroke risk factor. • - 60% of patients would contact their GP or NHS Direct if having a • stroke • - 75% of stroke patients misinterpret their symptoms. • - 86% of patients believe that their symptoms are not serious enough • to seek urgent care. • Just over half of GPs said they would refer someone with a suspected • stroke immediately. • 3. Hospital physicians’ lack of experience with stroke thrombolysis and therefore reluctance to ‘risk’ treatment. • < 12% of hospitals have protocols in place with ambulance services for • the rapid referral of those with suspected stroke. • < 50% of hospitals with acute stroke units have access to brain • scanning within three hours of admission to hospital.