CPC Case Conclusion
150 likes | 166 Vues
Explore a case of aspirin toxicity with hyperthermia and rhabdomyolysis, discussing ECG findings, acid-base imbalances, and important treatment interventions like hemodialysis. Learn about the significance of minute ventilation and mitigating acidemia in improving outcomes.

CPC Case Conclusion
E N D
Presentation Transcript
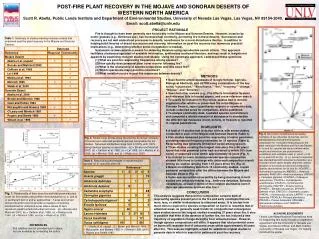
CPCCase Conclusion Aaron Schneir MD San Diego Division- California Poison Control System UC San Diego Medical Center
CPC Discussion The family brought in an empty bottle of…. Testing of previously drawn blood revealed a …… level of …..
Aspirin Salicylate level of 99 mg/dL!!!
CPCFurther Information History- suicide note with reference to ingesting aspirin; no history of excessive consumption of ephedrine-containing weight loss supplement Laboratory • Initial CK- 31,000 (explains AST elevation) • Comprehensive tox screen- ephedrine • Repeat UA- ketones present
CPCWhat about the initial ECG? Prolonged conduction secondary to hyperkalemia
Major clues to case 1) Hyperthermia 2) Worsening of condition with intubation
Aspirin and HyperthermiaUncoupling of oxidative phosphorylation Electron transport continues but without the coupled ATP synthesis. Result is heat generation.
Rhabdomyolysis and Salicylates Rhabdomyolysis = diffuse skeletal muscle necrosis Consequence of rhabdomyolysis • Acute tubular necrosis • Hyperkalemia
Salicylates and Rhabdomyolysis Mechanism 1) hyperthermia 2) increased muscular metabolism 3) compression of muscle 4) direct effect?
Acidemia and Salicylates pK = pH at which equal concentrations of an acid and its conjugate base are present pKa of salicylate = 3.5
Importance of Minute Ventilation with Salicylates Presence of acidemia allows for salicylate to penetrate brain CNS salicylate correlates with morbidity and mortality Essential to maintain minute ventilation to prevent acidemia
Improvement in Outcome 1) initial suspicion of salicylate overdose 2) attention to acid-base status and corresponding minute ventilation 3) rapid initial cooling 4) hemodialysis