Drug excretion
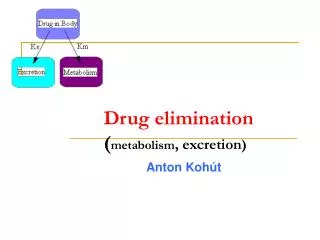
Drug excretion. Dr. S.O. Ogundele. Introduction. The elimination of drugs from the body involves the processes of metabolism and excretion Most drugs are metabolised first prior to being excreted

Drug excretion
E N D
Presentation Transcript
Drug excretion Dr. S.O. Ogundele
Introduction • The elimination of drugs from the body involves the processes of metabolism and excretion • Most drugs are metabolised first prior to being excreted • Some drugs, such as aminoglycoside are polar compounds and are excreted by the kidneys without being first been metabolised
Introduction • Definition • Drug excretion is the removal of drugs or drug metabolites from body fluids • It predominantly occurs via urine formed in the kidneys • Other routes of excretion of drugs from the body include • Bile • Saliva • Sweat • Tears • Faeces • Milk • Exhaled air
Basic kidney functions • The basic functions of the kidney include • Maintaining the volume and composition of body fluids • Controlling acid-base balance • Elimination of end-products of metabolism and foreign compounds (e.g., drugs)
Renal Extraction Ratio Renal Extraction Ratio • The fraction of a drug that is excreted when it passes through the kidneys is called the extraction ratio (ER) of the drug • A drug that is not excreted at all has an ER of 0 • A drug that is completely removed after a single passage has an ER of 1 • Extraction ratio: • Low (< 0.2):Acetazolamide, Chlorporpamide, Digoxin, Furosemide • Intermediate: Procainamide, Quaternary ammonia compounds • High: Glucuronides, Penicillins, Sulfates, Glycine conjugates
Renal clearance • Renal clearance • This is the hypothetical volume of plasma completely cleared of a particular substance (e.g. drug) per minute • As with the volume of distribution (Vd) of a drug, the renal clearance rarely corresponds to a physiological rate of flow that actually occurs
Renal clearance • Clearance (C) = UV/P • Where: • U = concentration in urine (mg/ml) • V = rate of urine flow (ml/min) • P = plasma concentration (mg/ml) • The units of clearance are ml/min • In order to make comparisons between species we may use ml/min/kg
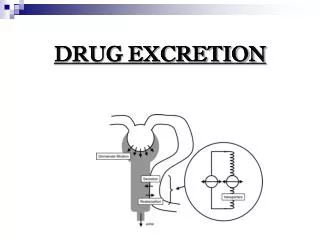
Mechanisms drug excretion by kidney • MECHANISMS of Renal Drug Elimination • Glomerular Filtration • Renal Tubular Secretion • Reabsorption by Non-Ionic Diffusion (passive) • Active Reabsorption
Mechanisms drug excretion by kidney • Drugs/metabolites are transported by the capillaries to the kidney tubule • Some drugs enter the tubule by glomerular filtration at the renal corpuscle • This acts like a sieve allowing small drugs and those not bound to plasma protein to filter from the blood into the Bowman’s capsule
Glomerular filtration • Glomerular filtration • Affects all drugs and metabolites of appropriate molecular size • Influenced by protein binding • Elimination is by first order process • Large drugs like heparin or those bound to plasma-protein cannot be filtered and are poorly excreted by glomerular filtration • Drug Filtration Rate = GFR x fu x [Drug] • fu = free fraction
Glomerular filtration • Regardless of mechanism, renal drug elimination declines in parallel with decreases in GFR • Therefore, CLCr canbe used to assess impact of renal impairment on renal excretion of drugs
Tubular Secretion • Most drugs do not enter the kidney tubule by glomerular filtration but do so by tubule secretion • In the proximal convoluted tubule active secretion of ionized drugs into the lumen occurs • This ensures that drugs which are protein-bound are excreted • It is energy dependent
Tubular Secretion • Active tubular secretion can be saturated, and drugs can compete for secretion • Tubule secretion involves two carrier systems • Basic carriers which transport basic drugs (amiloride, procainamide, dopamine, histamine) • Acidic carriers for acidic drugs (frusemide, penicillin, indomethacin)
Tubular Secretion • When therapeutic effect needs to be prolonged, agents can be co-administered to block tubular secretion • This will lead to the slowing of excretion of the drug e.g. penicillin with probenecid
Tubular Reabsorption • Despite glomerular filtration and active secretion renal clearance of many drugs is still slow because they are substantially reabsorbed from the distal portion of the nephron • Reabsorption of drugs can either be passive or active
Passive reabsorption • Passive reabsorption process is affected by the following factors • Concentration • About 99% of the water filtered through the glomerulus is reabsorbed in the kidney tubule • This results in a considerable concentrating effect which will lead to passive reabsorption • This is reduced by increasing the urine flow
Passive reabsorption • PH • Excretion of weak acids is increased significantly by alkalinizing the urine (sodium bicarbonate) • Excretion of weak bases is increased by acidifying the urine (ammonium chloride) • Lipid solubility • Highly lipid-soluble drugs are rapidly reabsorbed from the kidney tubule • Protein binding • Many protein-bound drugs are actively secreted into the proximal tubule, there is reabsorption of drugs that are largely protein-bound in plasma
Passive reabsorption • Passive reabsorption affects mainly weak acids and weak bases • E.g. • Weak Acids: Phenobarbital • Weak Bases: Quinidine • Important only if excretion of freedrug is the major elimination pathway • Ion trapping reduces reabsorption • Amphetamine (weak base, pKa9.2) is trapped in acidic urine, t1/2 7-34 hr • Ephedrine (weak base, pKa9.6) is trapped in acidic urine • Phenobarbital (a weak acid, pKa7.4) and salicylic acid(weak acid, pKa 3.0), are trapped in an alkaline urine
Active reabsorption • Affects ion mainly and a few drugs that are or resemble endogenous substances • E.g. • Halides: Fluoride, Bromide • Alkaline Metals: Lithium • Glucose • Salicylic acid(uric acid)
Effect of age on renal function • Infants • Glomerular filtration and tubular secretion are decreased in the newborn • Body water is increased in the newborn • Elderly • Glomerular filtration and tubular secretion are decreased in the elderly. • Glomerular filtration decreases 30 %from age 25 to age 65 and 48 %by age 90. • Tubular secretion decreases 38%from age 25 to age 65 and 62%by age 90
Effect of disease on renal function • Plasma protein binding decrease will increase the fraction of free drug and therefore the fraction available for filtration for some antibiotics • Renal blood flow decrease will decrease glomerular filtration (digoxin) and tubular secretion • Accumulation of drugs such as digoxin which are primarily eliminated by the kidney
Effect Of Drugs On Renal Function • Osmotic diuretics (mannitol) increase urine flow and reduce drug reabsorption • Nephrotoxic drugs (gentamicin) and heavy metals (Hg) reduce renal function • NH4Cl and NaHCO3 ion trap basic and acidic drugs, respectively, in the renal tubule • Probenecid reduces the secretion of penicillin and other anions
Restrictive Vs. Nonrestrictive Elimination • Restrictive • Clearance depends on protein binding • Kidney: Drug Filtration Rate = fU*GFR • Liver: CL = fU*Clint • Nonrestrictive • Clearance independent of Protein Binding • Kidney: CL = Q (renal blood flow)
Excretion from other route • Excretion in the Bile • This is the second most important route by which drugs and their metabolites are excreted • Large polar molecules (MW > 300) are often excreted in bile since they are not reabsorbed in the intestine • These drugs cannot diffuse across membranes and are therefore actively transported into bile
Enterohepatic Circulation • Drugs and drug conjugates entering the gut in bile may be reabsorbed and subsequently excreted in urine or returned to the bile • This occurs particularly with small, less polar drugs • Glucuronide conjugates of drugs may also be cleaved by enzymes in the intestinal microflora (e.g., beta-glucuronidase) to liberate the parent lipid-soluble drug, which is then reabsorbed
Excretion from other route • Saliva and Gut • Secretions from the saliva and gut play a small part in excretion • Bile is the major source of drugs excreted in the feces • Alveolar • This route is of major importance in the excretion of volatile anesthetics • The large surface area and rich blood supply ensure that equlibration between blood and alveolar air is extremely rapid • Milk • Excretion in milk is of particular concern in dairy animals