Acute Otitis Media
Acute Otitis Media. By Jennifer Naruta, RN. What is Otitis Media?. An acute infection of the middle ear Often follows eustachian tube dysfunction (ETD) or URI. Incidence of OM…. Most episodes occur in first 24 months of life 50% of infants in U.S. have first AOM before 6 months

Acute Otitis Media
E N D
Presentation Transcript
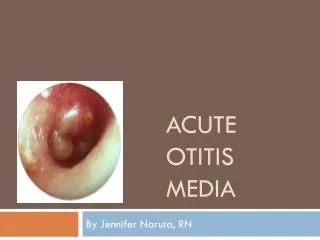
Acute Otitis Media By Jennifer Naruta, RN
What is Otitis Media? • An acute infection of the middle ear • Often follows eustachian tube dysfunction (ETD) or URI
Incidence of OM… • Most episodes occur in first 24 months of life • 50% of infants in U.S. have first AOM before 6 months • 65-90% of children will suffer at least one episode by age 2 • Most common indication for antibiotic prescriptions in U.S.
Etiology of OM • Children have shorter, more horizontal, more flaccid eustachian tubes • Easily disrupted by viruses • Predisposes them to AOM
Etiology of OM • Daycare attendance • Recent URI • Bottle Propping • Pacifiers • Asthma/allergies • Cleft Palate • Due to anatomical abnormalities • Down Syndrome • Due to anatomical abnormalities
Pathophysiology of OM • Usually arises as a complication of a preceding viral URI • Secretions and inflammation cause a blockage of the eustachian tube • Negative pressure is generated which pulls interstitial fluid into the tube • Serous effusion is created • Provides growth media for bacteria
Pathophysiology of OM • Organisms that cause OM include: • S. Pneumoniae (30-50%) • Prevnar vaccine decreases incidence of OM caused by S. Pneumoniae by 80% in children less than 2 years • H. Flu (15-30%) • M. Catarrhalis (10-15%) • RSV and Influenza most responsible for increase of AOM from January to April
Clinical Presentation • Acute onset otalgia • Infants/toddlers may pull at or play with ears • Irritability in infant or toddler • Fever • Disrupted sleep or inability to sleep • Dizziness/unsteady gait • Hearing loss (sudden) • Stuffy nose, rhinorrhea, sneezing
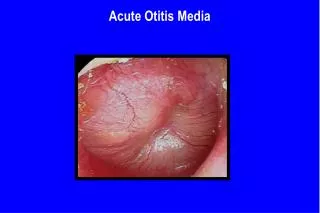
Diagnosis of OM by Physical Exam • AAP Guidelines require all three components for dx of AOM • Recent, abrupt onset of middle ear inflammation and effusion • Ear pain, irritability, otorrhea and/or fever • Bulging TM; limited or absent mobility by pneumatic otoscopy; air-fluid level behind TM; otorrhea • Erythema of TM or otalgia which interferes with sleep/activity
Diagnosis of OM by Physical Exam • Other TM findings may be present: • Increased vascularity • Obscured or absent landmarks • Red, Yellow, or purple color • Redness alone should not be used to diagnose AOM, especially in crying child
Differential Diagnosis • Mastoiditis • Dental abcess • Sinusitis • Lymphadenitis • Peritonsillarabcess • Trauma • ETD • Impacted teeth • TMJ dysfunction • Immune deficiency • Infants < 2mo with AOM should be evaluated for fever without focus and not just treated for an ear infection
Treatment Options • 80% of AOM cases will resolve on their own without antibiotics and without long term effects • “Watchful waiting” • Return if no improvement in 48-72 hours • For children > 6 months in absence of severe illness • Pain Management • Tylenol/Motrin • Benzocaineotic preparations (Auralgan) • For children > 5 without perforation • Anitbiotics • For all children < 6 months old • For children 6 months to 2 years with definitive diagnosis • For children over 2 years with severe illness
Treatment Options • Antibiotics • Amoxicillin • 1st line antibiotic for AOM • 80-90mg/kg/day divided in 2 doses • Augmentin • For severe illness (fever > 102.2 and severe otalgia) • 90mg/kg/day of amoxicillin with 6.4mg/kg/day of clavulante divided in two doses
Treatment Options • If Allergy to Amoxicillin • Nontype I reaction • Omnicef: 14mg/kg/day divided in 2 doses • Cefpodoxime: 10mg/kg/day in 1 or 2 doses • Ceftin: 30mg/kg/day divided in 2 doses • Type I hypersensitivity reaction • Azythromycin: 10mg/kg on day 1, 5mg/kg on day 2-5 • Poor coverage of H. Flu • Other possibilities • Erythromycin: 50mg/kg/day • Clindamycin: 30-40mg/kg/day in three divided doses • Ceftriaxone: 50mg/kg parenterally daily in 1-3 doses • For vomiting child • For child who has failed Augmentin after 3 days of treatment
Treatment Options • ENT Referral • After appropriate therapy has failed • Recurrent episodes of AOM • Pressure Equalizing Tubes (PETs) • Tympanostomy
Complications • TM perforation • Mastoiditis • Tympanosclerosis • Hearing loss of 25-30 dB • Ossicle necrosis
Prognosis • Prognosis is great • Symptoms usually improve in 24 hours and almost always within 72 hours • Educate parents and patients to finish all antibiotics if prescribed