Download
1 / 45
540 likes | 748 Vues
Slides prepared and compiled by highly experienced ENT teacher, Dr. Krishna Koirala from Nepal, for teaching undergraduate and postgraduate ENT students in the field of otorhinolaryngology. <br>A clear and concise explanation of the basic concepts in the subject matter concerned. <br>He is the Head of department with a sound knowledge in the field of ENT to teach both undergraduate and postgraduate ENT students

E N D
Acute Suppurative Otitis Media (ASOM) Dr. Krishna Koirala
Defined as pyogenic infection of middle ear cleft lasting for < 3 weeks • Routes for infection • Via Eustachian tube • Via Tympanic membrane perforation • Hematogenous (rare)
Predisposing Factors 1. Breast feeding in supine position 2. Recurrent upper respiratory tract infection 3. Nasal allergy 4. Chronic rhinitis & sinusitis 5. Tumours of nose & nasopharynx 6. Cleft palate
Bacteriology • Haemophilus influenzae • Streptococcus pneumoniae • Staphylococcus aureus • Moraxella catarrhalis • Beta hemolytic Streptococci (causative agent in acute necrotizing otitis media)
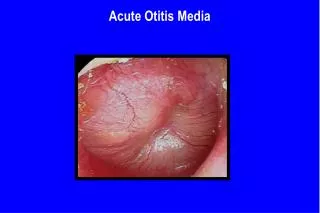
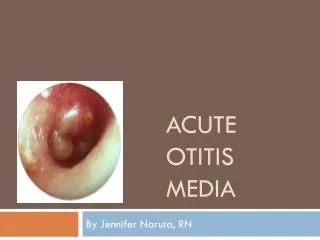
Stages of ASOM 1. Stage of hyperemia (tubal occlusion) • Mild earache • T.M. retracted initially and congested later • Blood vessels radiating out from handle of malleus (cartwheel appearance) Cartwheel
2. Stage of Exudation • High fever, severe earache, deafness • Marked congestion and bulging of T.M. • Mastoid tenderness • P.T.A. : high frequency conductive deafness (due to mass effect of pus)
3. Stage of Suppuration • Increased deafness, ear discharge • Mastoid tenderness + • Fever and earache decrease • Otoscopy : • Bulged, congested tympanic membrane with a yellow spot (nipple sign) • Pulsatile discharge through small TM perforation (Lighthouse sign)
4. Stage of Coalescent Mastoiditis • Otorrhea > 2 weeks, otalgia and deafness • Mastoid reservoir sign : pus immediately fills the EAC after mopping • Sagging of Postero-superior bony canal wall due to peri-osteitis of mastoid floor • Ironed out appearance of skin over the mastoid due to thickened periosteum • Mastoid cavity in X-ray due to hyperemic decalcification
5. Stage of Resolution • Ear discharge stops • Hearing improves • Perforation starts healing up
6. Stage of Complications • Sub-periosteal abscess • Vertigo • Headache + blurred vision + projectile vomiting • Fever + neck rigidity + irritability • Drowsiness • Paralysis of cranial nerve(s)
Treatment of ASOM • Antibiotic (Co-amoxyclav, Cefuroxime) • Nasal decongestants (systemic + topical) • H1 anti-histamines • Analgesic + anti-pyretic • Aural toilet for ear discharge • Heat application for severe earache
Review after 48 hours • Earache + fever persists: • Change to higher antibiotic • If T.M. is bulging perform myringotomy and send ear discharge for C/S • Earache + fever subside: • Continue same treatment for 10-14 days
Review after 3 months • No effusion • No further treatment • Effusion persists • Treat as Otitis Media with Effusion (OME) • Presence of abscess or coalescent mastoiditis • Cortical mastoidectomy
Myringotomy in A.S.O.M. • Curvilinear incision made in postero-inferior quadrant • Incision is curvilinear & not radial (as in OME), to cut the fibres of TM (to keep the opening patent for longer duration)
Why incision in PIQ? • Less vascular area • T.M. bulge is maximum • Ossicles not damaged • Easily accessible
Pathology Production of pus under tension hyperemic decalcification (halisteresis) + osteoclastic resorption of bone breakage of septa and formation of mastoid cavity sub-periosteal abscess penetration into periosteum + skin mastoid fistula formation
Abscesses related to mastoid • Post-auricular • Bezold • Citelli • Zygomatic • Luc • Retro-mastoid • Parapharyngeal & Retropharyngeal
Post-auricular abscess • Commonest • Present behind the ear • Pinna pushed forwards & downwards
Bezold’s & Citelli’s abscesses Bezold:neck swelling over sternocleido- mastoid muscle Citelli:neck swelling over posterior belly of digastric muscle
Luc: swelling in external auditory canal • Zygomatic:swelling antero-superior to pinna + upper eyelid edema • Retro-mastoid: swelling over occipital bone • Parapharyngeal & Retropharyngeal: due to spread of pus along the Eustachian tube
Gradenigo’s Syndrome Giuseppe Gradenigo (1859 – 1926)
Defining Triad • Persistent otorrhea despite adequate cortical mastoidectomy • Retro-orbital pain due to trigeminal nerve involvement • Diplopia: convergent squint due to lateral rectus palsy by injury to Abducent nerve in Dorello’s canal at the petrous apex
Etiology : Coalescent mastoiditis involving petrous apex along postero-superior & antero-inferior tracts in relation to bony labyrinth • Diagnosis: • C.T. scan temporal bone for bony details • MRI to differentiate b/w bone marrow & pus • Treatment:Modified radical mastoidectomy & clearance of petrous apex cells