Understanding Provider Payment Methods: Salary vs. Capitation
720 likes | 819 Vues
Explore how physician remuneration through salary and capitation impacts patient care quality, access, and physician incentives. Learn about the benefits and challenges of each method, along with strategies to mitigate adverse effects.

Understanding Provider Payment Methods: Salary vs. Capitation
E N D
Presentation Transcript
Paying the Physician Dr. Shahram Yazdani Shahid Beheshti University of Medical Sciences School of Medical Education Strategic Policy Sessions: 27
The principal methods of provider payment • Salary • Capitation • Fee-for-service • Case-based reimbursement
Salary • The most common system of physician remuneration • Physicians and other health care personnel are paid a fixed amount for predetermined hours of work. • The amount of salary does not depend on the number of patient visits, number of cases, severity of cases, etc.
Albania Bulgaria Croatia Estonia Finland Greece Lithuania Poland Portugal Romania Slovenia Sweden Turkey Salary Countries that follow a salary-based system for remuneration of health care personnel
Salary incentives • Salary-based remuneration systems provide almost no financial incentives to physicians for longer working hours, or seeing more patients, or spending more time and effort with each patient.
Salary Potential Impact on Patients • Salary-based remuneration system is likely to have both beneficial and adverse effects on the nature, quantity and quality of care that a patient receives.
Salary Beneficial Effects: • Physicians have no incentives to deny access to any patient. Since the compensation package is decided prospectively and is fixed, physicians have no reason to deny treatment to any patient. • Physicians have no incentive to provide excessive treatment, since the extent or type of treatment is not likely to alter their compensation in anyway.
Salary Adverse Effects: • Patients may not receive adequate attention from the physician, which may adversely affect patient satisfaction. • Access to care may be somewhat limited by the limited time that the physician may allocate to his duties. • Patients may potentially receive less than optimal care, and both quality and quantity of care may be compromised.
Salary • In the absence of incentives, performance becomes an ‘individual’ function that is not guided by ‘institutional' considerations.
Salary Administration • Probably the biggest advantage in the salary-based remuneration system lies in the ease and simplicity of administration. • There are no patient bills to be processed, no patient lists to be prepared, and no case-based groups to be formed.
Salary Administration • Physicians are treated like other employees of the administration, and their service records and payrolls maintained in the same manner. • Their promotions are usually time-based, like rest of the staff. • Personnel costs are known in advance, and can be built into any planning exercise of the health department.
Salary Measures to mitigate adverse effects of a salary-based remuneration system: • Governments/payers can offer non-pecuniary incentives to physicians,like awards, favorable posting, status-related designations etc. • Even pecuniary benefits can be built into a salary system. One example of such incentives are performance-related financial bonuses. • Governments/payers can set in place a system of quality control to monitor and maintain quality levels. • Governments/payers can improve monitoring to ensure greater availability of physician time.
Salary salary-based remuneration system
Capitation • Physicians and other providers receive a fee for each enrollee to cover a specified level of health care and offer a defined package of services, for a specified time period. • Physicians under capitation are usually responsible for all costs of providing the full package of treatment, including diagnostic tests, specialist consultations, and some minor, ambulatory surgery.
Capitation Geographic capitation • The physician receives capitation-based block funds to provide health care to the entire population in a given geographic area.
Capitation List capitation • The physician receives per-enrollee capitated funds to provide health care to all individual enrollees on a list.
Capitation Package of services • The defined package of services can include many different types of services. • Packages of services that include primary and family care are more common, since the cost of primary and family care is usually known with a high degree of certainty and the range of possible procedures is rather well defined and limited.
Capitation Capitation formula • The capitation formula is usually based on variables on which reliable information is available and easy to get.
Capitation Number of individuals Age Gender Marital status Socioeconomic conditions Urbanization Mortality and morbidity Number of individuals disabled Number of individuals under rehabilitation Number of individuals with substance abuse problems Epidemiological indices Variables commonly used in capitation formula
Capitation • Physicians thus receive a fixed amount per enrollee, and after meeting all costs of treatment, retain the surplus as their income.
Capitation • In some countries the principle of capitation is used to define provincial and district health care budgets. Fund allocation across different administrative areas follows use of capitation formulas that typically include demographic and epidemiological indices.
Capitation Countries that follow a capitation-based system for remuneration of health care personnel • Hungary • Ireland • Italy • Holland • Croatia (private sector)
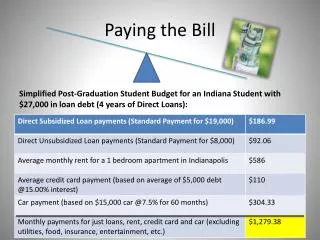
Capitation Example1 • The simplest capitation formula reimburses physicians according to the number of patients enrolled. Consider the case of Dr. A who has 2,836 persons enrolled on her list. The capitation formula used in her reimburses 5.50 $ per enrollee per month. • Calculation of compensation for Dr. A • Basic capitation remuneration: 2,836*5.50 = 15,598 $ per month.
Capitation Example2 • Dr. A has 2,500 persons on his list, of whom 1,500 are female and 1,000 male. Further, 500 persons are under the age of six, 1,500 are between 6 and 65, and 500 are above the age of 65. Dr. A has 16 years of experience. • Dr. B has less than 1 year of working experience. She has 3,000 persons on her list, of whom 2,000 are female and 1,000 are male. Further, 400 persons are under the age of six, 2,000 are between the ages of 6 and 65, and the remaining 600 over 65.
Capitation Example2 (ctd.) • The monthly capitation formula awards 1 point per enrollee for the first 2,500 enrollees, and 0.5 points per enrollee thereafter. • Enrollees below the age of 6 and above the age of 65 are awarded an additional 0.5 point each. • Female enrollees are awarded an additional 0.1 points. • Physicians with more than 10 years of experience are awarded an additional 2% for every additional year of experience. • Each point is worth 1$
Capitation Example2 (ctd.) • Calculation of compensation for Dr. A: • Basic capitation fee: 2500*1 = 2500 • Age-specific additions: (500*0.5+500*0.5) = 500 • Gender-specific additions: 1500*0.1 = 150 • Total: = 3150 • Experience bonus: (16-10)*0.02=12% = 378 • Grand total = 3528
Capitation Example2 (ctd.) • Calculation of compensation for Dr. B: • Basic capitation fee: 2500*1+500*0.5 = 2750 • Age-specific additions: (400*0.5+600*0.5) = 500 • Gender-specific additions: 2000*0.1 = 200 • Total: = 3450 • Experience bonus: nil = 0 • Grand total = 3450
Capitation Incentives • Capitation provides a number of financial and professional incentives to the physicians. Some of these are positive and beneficial incentives while others are adverse.
Capitation Beneficial Incentives: • Physicians have strong incentives to minimize financial costs. Since the compensation package is decided prospectively, physicians can maximize the difference between their earnings and costs by simply keeping costs down. • Physicians have strong incentives to make efficient the whole episode of care. Preventive medicine that is likely to save expensive treatment later on is thus favored.
Capitation Adverse Incentives: • Physicians have an incentive to enroll relatively healthy patients, who are likely to require less frequent and less costly treatment. • Physicians have an incentive to limit the quantity of services provided to the patient, as this would reduce their operating costs.
Capitation Adverse Incentives: • Physicians have an incentive to save on high quality treatment, since such treatment is usually expensive. • Physicians have an incentive to refer patients to next higher levels of care, such as to specialists and hospitals, so as to save own operating costs
Capitation Potential Impact on Patients • A capitation-based remuneration system is likely to have both beneficial and adverse effects on the nature, quantity and quality of care that a patient receives.
Capitation Beneficial Effects: • In many capitation-based settings, the patient receives most kinds of care from the same physician. Besides being convenient, it also strengthens the relationship between the physician and the patient. • The patient is likely to receive only those services and interventions that are necessary. Over-treatment and unnecessary interventions are unlikely in this system.
Capitation Adverse Effects: • Patients requiring many and complex treatments may be excluded from the enrollment lists of physicians receiving capitation-based remuneration. • Patients may potentially receive less than optimal care, since the physician has an incentive to keep costs down. Both quality and quantity of care may thus be compromised. • In many capitation-based settings, it is not easy and straightforward for the patient to change her physician.
Capitation Administration • The capitation system requires little administration, as there are no patient billsto be processed. Once the lists are finalized, computing an individual physician's reimbursement does not require many calculations. • Health expenditures under this system are entirely predictable, and there is good control over costs.
Capitation Administration • However, governments and payers may incur high administrative costs in preparing and maintaining the list of enrollees. • High administrative costs are also associated with negotiating contracts, setting capitation rates and formulas, and monitoring physicians to ensure that appropriate levels and quality of care are being provided to the patients.
Capitation Measures to mitigated the adverseincentives facing the physicians: • Governments/payers can mandate open enrollment, such as across a given geographical or administrative area. This prevents the physicians from selecting the relatively healthy patients into their pool. At the same time, the potential risk to the physicians is also minimized, since spreading the base from which to select enrollees reduces the chances of relatively unhealthy members dominating the pool.
Capitation Measures to mitigated the adverseincentives facing the physicians: • Governments/payers can encourage competition among physicians. If the patients have the choice to periodically select their physicians, the potentially adverse consequences for quantity and quality of care can be overcome.
Capitation Measures to mitigated the adverseincentives facing the physicians: • Governments/payers can define the package of services to include many (not necessarily all) such services that are usually provided at a next higher level. Thus, if family care physicians are required to provide diagnostic services as well, there will be fewer incentives for the physician to refer patients for additional tests. Similarly, if visits to a specialist are covered by the physician as part of the capitated services provided, there will be fewer incentives to refer patients to specialists.
Capitation Measures to mitigated the adverseincentives facing the physicians: • Governments/payers should set in place a system of quality control and monitoring so as to mitigate the adverse incentive that the physician faces of compromising on quality.
Capitation Capitation-based remuneration system
Fee-for-Service • Under this system the physician and other workers are reimbursed according to the number and type of different services provided to the patient. • A specific price is set for each service, which may be fixed or variable.
Fee-for-Service • In the fixed system, the physician and the payer agree to a schedule of rates at the beginning of the year, and all bills within the agreed time-period are based on this schedule. • In the variable system there is no such schedule, and the physicians and other healthcare personnel charge the current usual and customary fee.
Germany (private physicians and dentists) Belgium Czech Republic France Switzerland Ireland (private sector) Holland (private sector) Bulgaria (private sector) Greece (private sector) Slovenia (private sector) Turkey (private sector) Fee-for-Service Countries that follow a Fee-for-Service system for remuneration of health care personnel
Fee-for-Service Incentives for Physicians • Fee-for-service provides a number of financial and professional incentives to the physician. Some of these incentives have a beneficial impact while others have an adverse impact.
Fee-for-Service Beneficial Incentives: • Physicians have strong incentives to increase both the production and quality of health care. Thus, the physician is likely to see more patients and provide many services, which is likely to be satisfying for most consumers.
Fee-for-Service Adverse Incentives: • Physicians have a strong financial incentive to increase the volume of services, even to levels higher than required. This is likely to increase total spending on health care. • Physicians have a strong incentive to induce demand. Consumers of health services tend to base their decisions of health care needs on the advice given by the providers. Since the providers have an incentives to increase the volume of services, there may be a tendency to oversupply and overuse services.
Fee-for-Service Potential Impact on Patients • Fee-for-service based remuneration system is likely to have both beneficial and adverse effects on the nature, quantity and quality of care that a patient receives.
Fee-for-Service Beneficial Effects: • The patient is likely to receive optimal level and quality of care, though there is always the risk of over-treatment and unnecessary interventions. • Patients requiring many and complex treatments are not likely to be excluded from receiving care. • It is relatively easy and straightforward for the patient to choose and change physicians at any point.
Fee-for-Service Adverse Effects: • The biggest risk for the patient is that the physician may prescribe excessive treatment and interventions. This phenomenon, also known as “supplier induced” demand, is observed to be widespread in countries where physician remuneration is based on fee-for-service.