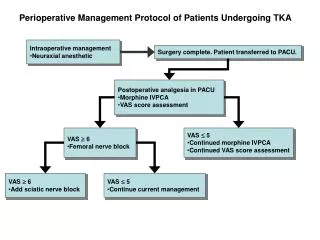
Primary TKA
Primary TKA. Beom Koo Lee, M.D. Dept. of Orthopaedic Surgery Gachon University, Gil Medical Center. CR or PS. Advantage of CR. Maintain central stabilizer Maintain joint line Conservation of bone Patella clunk syndrome Avoidance of the Stress Inherent in


Primary TKA
E N D
Presentation Transcript
Primary TKA Beom Koo Lee, M.D. Dept. of Orthopaedic Surgery Gachon University, Gil Medical Center
Advantage of CR • Maintain central stabilizer • Maintain joint line • Conservation of bone • Patella clunk syndrome • Avoidance of the Stress Inherent in Posterior Cruciate-Substituting Knees • Ease of Management of Supracondylar Femur Fractures Insall surgery of knee
Trend in USA CR PS • 1995 85% • 2001 46%
Draw back of CR • Perfect PCL balance can’t be obtained predictably Dennis1996 CORR 331
Shearing in deep flexion Shearingin CR
Drawback of CR • PCL function is compromized as a result of the degenerative process involving knee Lombardi CORR 2001 ;392:75-87 Ranawat CORR 1994;309:131
Drawback of CR Marked lift off in CR • Dennis CORR 410’2003 P 114
Drawback of CR • paradoxical sliding and opposite rotation in CR • near normal roll back in PS Fluoroscopic exam of fixed bearing TKA Dennis CORR 410’03 P114
Draw back of CR • Early loosening with osteolysis in CR Which is very rare in PS Agilietti 1996 AJKS Colizza 1995 JBJS 77-A;1713
Drawback of CR • Better ROM in PS Delp1995 ,Kochmond 1995 J Arthroplasty • Easy rehab in PS type 정현기
Drawback of CR • TKA CR In RA instability in 15% (posterior instability, recurvatum, mediolat instability) (Meding 2004 CORR428 P146)
Drawback of CR Hyperextension and anterior displacement in CR 슬관절 전치환술에서 경골 후방 경사각이 인공 슬관절의 안정성에 미치는 영향 서재곤
Advantage of PS • The deformity can be corrected easily. • Minimal tibial resection is possible. This allows placement of the tibial component in stronger host bone • Knees have more normal kinematics • Polyethylene wear is decreased when a conforming articular John J. Callaghan Insall Surgery of knee
Advantage of CR • patients with PS knees reportedgreater functional limitations in squatting, kneeling, and gardening. • Our results suggest that with the specific implant used in this study, substitution for the PCL with a spine and cam mechanism may not fully restore the functional capacity of the intact PCL, particularly in high-demand activities that involve deep flexion. Conditt J Arthroplasty Oct‘2004 P 107
Algorithm PS CR • RA, prior patellectomy Prior HTO prev PCL rupture • Grade II-III flexion contracture • Deformity greater than 15 • Severe disease • Incompetent PCL • deformed,deficient, contracted, laceration, excessive recession Grade I flexion contracture deformity less than 15 Moderate disease Competent PCL Intact , balanced PCL Lombardi CORR 2001 ;392:75-87
PS Joint space narrowing (+) Femoral & tibial condyle erosion (+) Bony spurs: + Moderate deformity Posterior contact
PS Postslope more than 7
CR Tibia posterior slope less than 7 Contact point more than posterior 1/3 Less deformity
Patella resurfacing or not Patellar resurfacing, perhaps more than any other area of TKA, as been surrounded by controversy in the 30 years of its existence
3 camp • patellar resurfacing as a routine part of TKA, • others continue to avoid resurfacing the patella, • "selective resurfacing of the patella
Favor resurfacing • Better pain relief Extensor mechanism complication after TKA (James Rand ICL'05 P241)
Long-Term Changes of the Nonresurfaced Patella After Total KneeArthroplasty Favor resurfacing • Progressive degenerative changes of the nonresurfaced patella in 40% Hsin-Nung Shih, J. Bone Joint Surg. Am., May 2004; 86: 935 - 939.
Favornon resurfacing Scott F. Dye, Geoffrey L. Vaupel, and Christopher C. Dye Am J Sports Med Nov 1998 26: 773-777.
Favor non resurfacing • No significant difference was found regarding these revision rates or the Knee Society clinical rating scores, functional scores, patient satisfaction, anterior knee pain, or radiographic outcomes Burnett RS, Haydon CH, Rorabeck CH, et al. Clin Orthop 428:12, 2004. Barrack RL, Wolfe MW, Waldman DA, et al: J Bone Joint Surg Am 79:1121, 1997 Feller JA, Bartlett RJ, Lang DM:. J Bone Joint Surg Br 78:226, 1996
Favor nonresurfacing • High complication rate and questionable benefits associated with resurfacing John Gallagher Insall surgery of knee James Rand ICL'05 P241 Extensor mechanism complication after TKA
Favor selective resurfacing • Progressive degenerative changes of the nonresurfaced patella (mainly on the lateral facet) and patellar maltracking were the most common abnormal radiographic changes. • Patients with preoperative patellar maltracking were at risk for the development of these changes and clinical symptoms. • Resurfacing of the patella during total Knee arthroplasty may benefit such patients. Hsin-Nung Shih, J. Bone Joint Surg. Am., May 2004; 86: 935 - 939.
Selective resurfacing Pre-op ant knee pain Inflammatory arthritis Advanced chondromalacia Obesity Malalignment Lack of congruency Extensor mechanism complication after TKA (James Rand ICL'05 P241)
Patella unresurfacing Bone Inactive patient Minimal OA Small patella
Patella resurfacing Bone • Tibiofemoral F/53 RA
Patella resurfacing Pat grade IV OA with pain Maltracking Active age
Tibia 1 st or femur 1 st Gap techn or Measured resection
Essential philosophy of the gap technique • It builds on the state of the soft tissues • The soft-tissue correction is performed first and the measured gap resection is performed next. Insall 4th
Gap techn; Tibia cut • cut at right angles to the long axis in the coronal plane (A) • Posterior slope; 0-5 Insall 4th
posterior femoral cut; Size and rotation After tensioning, the size and rotation is determined
Classic measured resection technique Replace a bone with prosthesis So the cut bone should be identical size with prosthesis thickness
Measured resection techn Distal femoral cut; alignment 90 to mechanical axis from the center of the femoral head to the center of the knee In practice the intramedullary alignment rod is inserted and distal cutting guide matching the pre-op determined angle ( normally aligned in 6 to 7 degrees of valgus) is applied. Insall 4th
Prosthesis thickness (9mm) Measured resection techn Distal femoral cut ;depth of cut Figure 84-24 Ideally, the amount of distal femoral resection should be judged from the normal side. Insall 4th
Bone size determined by sizer The size usually match to Prosthesis thickness (9mm) Measured resection techn prosthesis size and depth of posterior femoral cut Insall 4th
My practice; combination • Measured Resection; proximal tibia and distal femur • Ligament balance in extension • Gap Techniques rotation & size
Femur 1 st Huge posterior bone spur that block anterior displacement of tibia
Advantageof high flexion • although the degree of postoperative knee flexion did not affect patient satisfaction, it did influence fulfillment of expectations, functional ability, and knee perception. Brandon N. Devers, Michael A. Conditt, Miranda L. Jamieson, Matthew D. Driscoll, Philip C. Noble, Brian S. Parsley Does Greater Knee Flexion Increase Patient Function and Satisfaction After Total Knee Arthroplasty? JA feb 2011 Pages 178-186