A Case Study of a Simulation-Based Decision Support Tool
190 likes | 322 Vues
This case study, conducted by the University of Toronto's Healthcare Resource Modeling Lab, explores a simulation-based decision support tool aimed at optimizing cardiac surgical resource allocation at Hamilton Health Sciences Centre. The study addressed the challenges of expanding operating room activity, ensuring adequate ICU and ward bed availability, and minimizing surgery cancellation rates. Through various simulation scenarios, the tool provided insights to improve scheduling efficiency and meet provincial surgical targets, thereby enhancing clinical operations.

A Case Study of a Simulation-Based Decision Support Tool
E N D
Presentation Transcript
A Case Study of a Simulation-Based Decision Support Tool Michael Carter Healthcare Modeling Lab, Mechanical & Industrial Engineering, University of Toronto ORAHS 2006: Poland
Organizations Involved • University of Toronto • The Health Care Resource Modelling Lab • Hamilton Health Sciences Centre (HHS) • Perioperative Services • Clinical Appropriateness and Efficiency Program (CARE) • Institute of Clinical Evaluative Sciences ORAHS 2006: Poland
Primary Team Members • University of Toronto • Jean Yong – MASc candidate • Michael Carter – Director, Healthcare Resource Lab • Carolyn Busby – Doctoral Candidate & Modeller • Hamilton Health Sciences • Kelly Campbell – Director of Perioperative Services • Steve Metham – CARE Facilitator • Dr. Kevin Teoh – Head of Cardiac Surgery • ICES • Dr. Jack Tu – Senior Scientist ORAHS 2006: Poland
Background • Background: • Expansion of operating room activity • Determine new surgical booking policy • Objective: • Facilitate strategic planning of cardiac surgical resource allocation • Determine OR schedule • Determine number of beds required in ICU and ward ORAHS 2006: Poland
No Redo/ Combined Surgery Grouping Cardiac Surgery 2002-2004 N>4000 Redo/ Combined CABG VALVE COTHR CONGD CABG VALVE AORTA CAVLV AORTA CAVLV COTHR CABG 1,2,3 TVR,AVR CONGD COTHR CABG 4,5,6,7 MVR ORAHS 2006: Poland
Surgery Grouping Cardiac Surgery 2002-2004 Major 1 353 mins n=116 Major 2 431 mins n=60 Intermediate 322 mins n=281 359 Minor 244 mins n=1016 266 In-btwn 284 mins n=890 313 ORAHS 2006: Poland
Minor 246 mins n=1530 In-btwn 285 mins n=1789 Major 461 mins n=220 Intermediate 337 mins n=499 Surgery Duration Distribution ORAHS 2006: Poland
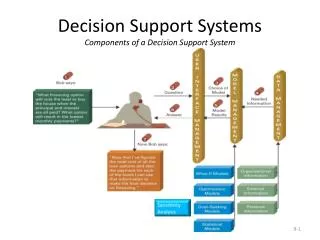
Conceptual Model Queue by surgeon Surgery duration – by procedure Waiting List Prioritized by acuity Cardiac Surgical Unit Operating Room ICU Cardiac Surgical Unit Same Day Surgery Ward Discharge ORAHS 2006: Poland
Performance Indicators • Number of cases completed/year • Cancellation rates • Lack of ICU/ ward bed • Out of scheduled time • More urgent case took precedent • Operating room utilization • Under-utilization (hours/week) • Overtime (hours/week) • Ward bed utilization (ICU & CSU) ORAHS 2006: Poland
Model Validation • 50 replications of 1 year each • Imitate current scheduling rules • Run the model with 2002, 2003, 2004 data • Compare output from the 3 models with historical data • Experts’ opinions • Meeting with clinicians ORAHS 2006: Poland
Results ORAHS 2006: Poland
Applications Can we meet provincial target with 4 ORs varying room length Do we have enough ICU/ ward capacity? What if we pool all the surgeons’ urgent slots together? • Simulated what-if scenarios for 4 operating rooms to answer stakeholders’ questions • Encouraged clinicians to propose new ideas of how the system could be run differently for higher efficiency • Tested over 10 scenarios Can we book surgery differently? ORAHS 2006: Poland
Key issues from surgery • Ability to achieve priority funded volumes • Organization of block time – length and placement • Available beds – ICU/ward • Minimizing cancellation rate • Booking rules • Pooling of referrals • System for urgent/emergent cases ORAHS 2006: Poland
Modifying Cancellation Rule ORAHS 2006: Poland
Can we book surgery differently? ORAHS 2006: Poland
Scenario A Scenario B Scenarios – OR schedule ORAHS 2006: Poland
Model Results ORAHS 2006: Poland
Planning ICU and Ward Capacity ORAHS 2006: Poland
Questions? ORAHS 2006: Poland