Download
1 / 45
450 likes | 820 Vues
G Jondeau Centre de référence syndromes de Marfan et apparentés Hôpital Bichat 75018 www.marfan.fr. A quoi est dû le syndrome de Marfan ?. Elastic fiber. Microfibrils. Circulation. 2002;106:900. Desorganisation fibres élastine. Fibres elastine en vert : Marfan.

E N D
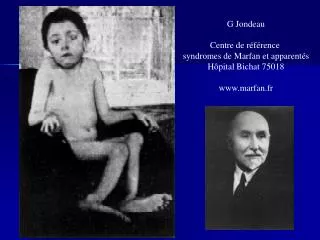
G Jondeau Centre de référence syndromes de Marfan et apparentés Hôpital Bichat 75018 www.marfan.fr
Elastic fiber Microfibrils
Desorganisation fibres élastine Fibres elastine en vert : Marfan Fibres elastine en vert:normal
Importance des MMP Control, MMP-7 MMP-7 Mucoid degenration Control, MMP-3 MMP-3 Mucoid degenration Human Pathology 2008
Difficile : grande variabilité Circulation (in press)
De Paepe Am J Human Genet 1996;62:4173 systèmes, 2 critères majeurs (18 ans) Génétique: Parent MFS, mutation pathogène FBN1, linkage à FBN1 (1) Cardio-vasculaire Dilatation ou dissection de l ’aorte ascendante (1) PVM±IM, Dilat AP (<40 y.o.), Ca anneau M < 40 y.o., Dilat ou dissec Ao descend thor ou abdo < 50 ans (1) Oculaire ectopie cristallin, cornée plate, longueur axiale globe, myosis (2) Squelette (2 M ou 1M + 2m): M (>4):Pectus carinatum ou chirurgical, SI/SS > 1.05, poignet et pouce, Scoliose > 20° spondylolistesis, coudes<170°, pied plat: m: Pectus modéré, Hyperlaxité, palais arqué, aspect Pulmonaire: pneumothorax, bulles apicales (1) Dure mère: ectasie dure-mère lombo-sacrée (scanner ou IRM) Peau: vergetures, hernies récidivantes ou sur cicatrice (1)
15 29 56 Intérêt Biologie moléculaire 10 12 78 J Med Genet 2008
N. Paganini A. Lincoln Aménophis IV S. Rachmaninov
Sur quoi est-on d’accord ? • Limitation des sports isométriques • Prophylaxie endocardite • Traitement béta-bloquant • Inhibiteurs calciques si intolérance • ? IEC (inefficaces ?) • ? Sartan (inefficaces ?) • Chirurgie préventive
ß blockade > 11 y.o. HR < 100 bpm exercise Controlß- death 2 0 Dissec 4 2 AR 2 2 >6cm 1 1 Total 9/38 (23%) 5/32 (16%) Shores N Engl J Med 1994;330:1335-41
60% 55% 45% Percentage of patients 35% 35% 30% 20% 10% 5% 5% ≤ 31 ≤ 33 ≤ 35 ≤ 36 ≤ 37 ≤ 41 ≤ 43 ≤ 47 surgery 50 Aortic diameter at Valsalva sinus (mm) Dissection descendante ESC 2009
Mouse C1663R cystein within cbEGF-like domain No clinical or histologic features of MFS Immunohistochemistry: presence of human epitope : bioavailability and competence of cysteine-substituted fibrillin-1 to participate in microfibrillar assembly Mouse C1039G cystein within cbEGF-like domain Clinical and histologic features of MFS Modèle animal : souris KI Judge J. Clin. Invest. 114:172–181 (2004)
Voie TGB-béta… Post natal TGFB antibody Habashi JP Science 2006;312:117
Voie TGF-béta, sartan ? Post natal TGFB antibody Habashi JP Science 2006;312:117
USA Losartan vs Atenolol: randomised open label Atenolol : HR by 20% on Holter (max 250 mg) Losartan: 0.4 mg/kg (max 100 mg) France Losartan on top of ttmt randomised double blind 10 yo and older 50mg if <50 kg 100 mg if > MARFAN-SARTAN Etudes en cours dans le syndrome de Marfan
mort subite Bentall morts subitesarbre complet 29 27 35 39 57 47 35 9 Nature Genet 2006
Syndrome de Loeys Dietz NEJM 2006;355:8
Survie TGFBR2 vs FBN1cohortes (n=90, 293) P=0.0216 Circulation (in press)
Survie TGFBR2 vs FBN1groupes (n=71, 243) Circulation (in press)
gène en 16p13 : MYH11 protéine : myosine ch.lourde FTAA et persistance du canal artériel FTAA4 (OMIM #132900) Khau Van Kien, Eur J Hum Genet, 2004, 12:173 Zhu, Nat Genet, 2006, 38:343
Diversité des étiologies & monotonie des phénotypes syndromiques dégénératifs fibrilline/TGFbR/myosin/Acta 2/notch-1/Glut 10 molécules cellules apoptose CML dégénérescence mucoide protéases tissue dégradation de la matrice anévrysmes dissections clinique registres/familles informatives/ biothèques (plasmas, tissus, cellules) critères de substitution/essais thérapeutiques
Conclusions • Monotonie du phénotype • pas de diagnostic étiologique histologique • Gènes : multiples • FBN1, TGFBR1, TGFBR2, prot contractiles • Enquête familiale • Tous les anévrysmes ! • Progrès thérapeutiques en vue ?


![[Nom de l intervenant] [Nom de l h pital]](https://cdn4.slideserve.com/1126866/slide1-dt.jpg)