Is there a consensus view on what is PCOS
520 likes | 785 Vues
Is there a consensus view on what is PCOS. M. Aboulghar Cairo, Egypt. A click on pubmed. PCOS: 3655 articles PCO: 2745 articles This large number of articles suggests: It is a common problem. It is an important condition.

Is there a consensus view on what is PCOS
E N D
Presentation Transcript
Is there a consensus view on what is PCOS M. Aboulghar Cairo, Egypt
A click on pubmed • PCOS: 3655 articles • PCO: 2745 articles • This large number of articles suggests: • It is a common problem. • It is an important condition. • There are more controversies and grey areas rather than solid facts.
I shall try to answer the following questions: Is there a consensus on prevalence? Is there a consensus on aetiology and pathogenesis? Is there a consensus on diagnosis? Is there a consensus on treatment? Is there a consensus on prognosis?
Polycystic ovary syndrome (PCOS) is the most common, yet complex endocrine disorder affecting women in their reproductive life(Abbott et al 2002)
Prevalence Wide variation in the reported incidence: why? Influenced by population studied. Selection bias. Diagnostic criteria.
Based on ultrasound criteria 17-27% Polson 1988 14-30% Tayob et al 1990 16-28% Clayton et al 1992 14-27% Farquhar 1994 14-19% Botsis et al. 1995 33% (Michelmor et al 1999) 23% Lowe et al 2005
Based on geographical distribution 5% in the US 33% in the UK(Agrwal et al 2004)
Based on naked eye observation of 12160 laparotomies conducted in women in reproductive age, PCO were reported in 1.4% (Vara and Niemineva 1951)
Prevalence of PCOS The incidence was14% among heterosexual subfertile population and 32% in Lesbian women (Agrwal 2004)
Is there a consensus on aetiology and pathogenesis of the syndrome?
Onset and pathogenesis of PCOS Genetic factors. Factors in utero. Environmental factors.
PCO has an extremely heterogenous clinical picture and is multifactorial in aetiology (Zawadski and Dunaif 1992)
Cytogenetic studies failed to demonstrate a specific gene disorder in PCOS. However, specific gene analysis showed different altered patterns of expression suggesting genetic origin (Diamauti-Kandarakis and Paeri 2005)
There is increasing evidence to support a major genetic basis for PCOS Strongly familial (Franks et al 1997). Search for a single gene is ongoing. Possible clustering genes (Urbanek et al 1999).
Earlier development of PCOS PCOS may develop during the second or first trimester of intrauterine life (Abbott et al 1998). Exogenous excess androgen creates PCOS pattern in adulthood of experimental animals. (Abbott et al 1998).
Excess androgen during pregnancy on fetus in utero Exogenous androgens are likely to affect human fetus in utero (MacClamrock and Adashi 1992). Hyperandrogenic fetal ovary (Payne and Jaffe et al 1974) or hyperandrogenic adrenal cortex (Barnes et al 1994) may reprogram multiple organ systems that will latter manifest in the heterogenous type of PCOS.
Eisner et al (2002) have shown that early in utero exposure to androgen exceeds in female rhesus monkey leads to improvement in insulin secretion, whereas exposure in late gestation causes impairment in insulin action
Stein and Leventhal reported the original description of PCOS in 1935.Since then tens of definitions and variable combination of manifestations represented polycystic ovarian disease.
Polycystic ovaries is purely description of ovarian morphologyorPCOS is a syndrome
Original diagnosis of polycystic ovarian disease Stein Leventhal 1935 Excessive androgen manifestation (Hirsutism, Achne) Obesity Oligomenorrhea or amenorrhea. Enlarged ovaries with thickened Tunica during laparotomy.
North American viewbased on NIH conference (1990) Combination of oligoamenorrhea or amenorrhea. And or clinical or biochemical evidence of hyper androgenemia. Absence of adrenal hyperplasia, hyperprolactinemia and thyroid dysfunction. Ultrasound appearance of ovary was not included.
European view 1995Menstrual disturbance In a large study of 1971 PCO patients (Balen et al 1995): 50% had oligomenorrhea 20% had amenorrhea 30% regular mensus.
European view (Balen 1999) Polycystic ovaries on ultrasound examination together with some of the following features: Androgenous manifestation. Obesity. Oligomenorrhea or amenorrhea. Elevated LH hormone.
Metabolic syndrome Hyperinsulinemeia, obesity, dyslipidemia, hypertension, atherosclerosis, increase risk of type II diabetes and coronary heart disease. Is two fold higher than age matched women in general population (Apridonidze et al 2005) Should we investigate all women for these risk factors?
Body weight and PCOS • Over 50% of PCOS are overweight (Gambineri et al 2002). • Less than half of PCOS patients are lean.
What is the role of insulin in PCOS? Only half of women with the diagnosis of PCOS have insulin resistance (Ajayl and Ogunmokum 2007). Should we test for insulin resistance in all patients?
Hyperandrogenism (clinical) Hirsutism: Informative data in large population is lacking. Subjective assessment. No routine standard scoring methods. Hirsutism may be treated before evaluation for PCOS. Racial variation.
Over 50% of PCOS are overweight (Gambineri et al 2002). • Less than half of PCOS patients are lean.
Measurement of LH • LH levels should not be considered necessary for clinical diagnosis of PCOS. • LH could be useful as a second parameter (Rotterdam 2003).
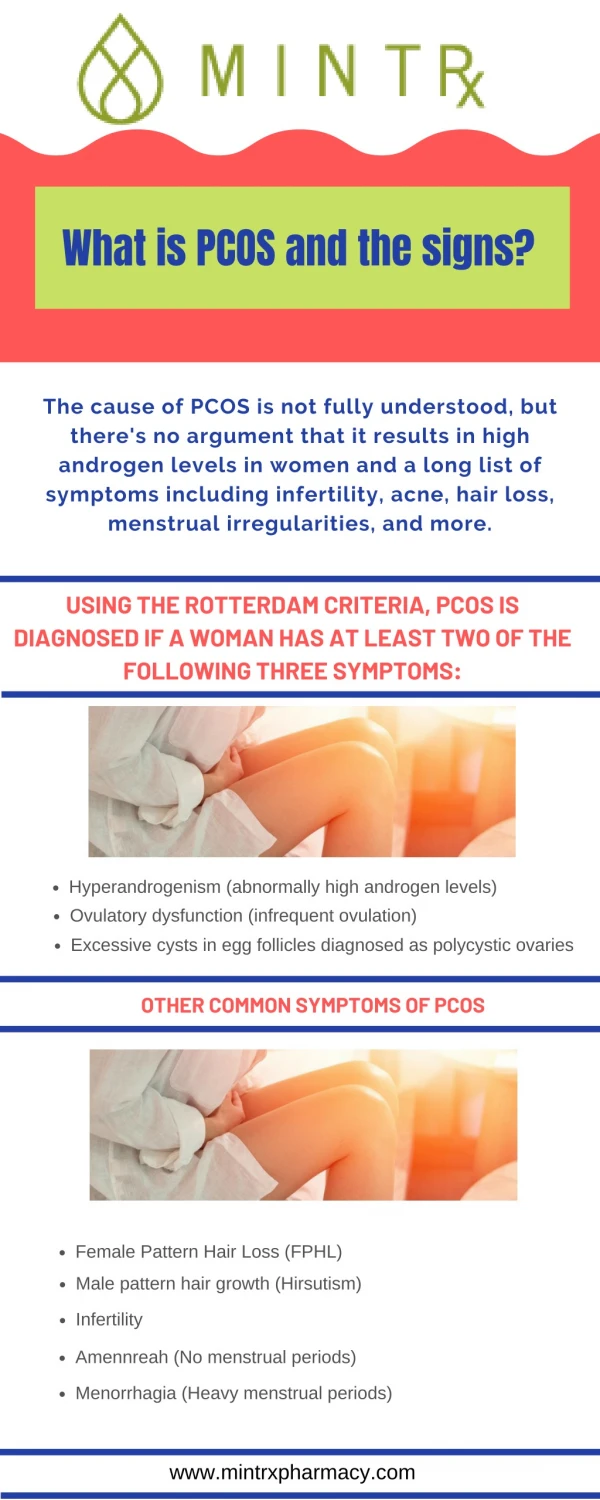
Rotterdam ESHRE-ASRM consensus 2003 • Oligo- and/or anovulation. • Clinical and/or chemical signs of hyperadnrogenism. • Polycystic ovaries. Two of these items and exclude other etiologies (Congenital adrenal hyperplasia, androgen secreting tumors, Cushing’s syndrome).
Rotterdam criteriaPCO ultrasonic criteria • Presence of 12 or more follicles each ovary measuring 2-9 mm • And/or increased ovarian volume (> 10 ml)
Answer: No It is a condition that may not require medical treatment as symptoms may be ameliorated by simply changing life style (Norman et al 2002) However, 50% of patients have a normal BMI.
Is there a consensus on the use of metformin for treatment of PCO?
Clomiphene, metformin or both for infertility in PCO patientsLegro et al (NEJ 2007) For 6 months
Comment • Clomiphen is superior to metformin in treatment of infertility associated PCO. • Adding metformin to clomid did not significantly improve pregnancy rate.
Clomid + metformin vs. clomid + placebo Moll (BMJ 2006) randomized multicenter Dutch study 228 women with PCO for 6 months
Comment • Metformin is not an affective addition to clomid in ovulation induction for PCO. • It seems that Metformin alone is not effective in ovulation induction for PCO.
Use of metformin for ovulation induction in PCOS: a meta- analysis (Creanga et al 2008) • 17 met criteria for inclusion • Metformin improved the odds of ovulation in women with PCOS when compared with placebo (OR 2.94; 95% CI 1.43-6.02; NNT 4) and appears more effective for non-clomiphene-resistant women. • Metformin increased the likelihood of ovulation (OR 2.67; 95% CI 1.45-4.94; NNT 4.6) when compared to CC alone. • Using all available evidence, this meta-analysis suggests that metformin increases the likelihood of ovulation and in combination with clomiphene, increases the odds of both ovulation and pregnancy in women with PCOS.
Metformin treatment before and during IVF in women with PCO (Tso et al 2009) • No evidence that metformin improved live birthrates (3 RCTs) OR 0.77 (95% CI 6.27-2.18). • No evidence that metformin improved clinical pregnancy rate (5 RCTs) OR 0.71 (05% CI 0.39-1.28). • Risk of OHSS is significantly reduced OR 0.27, 95% CI 0.16-0.47).
Is there any consensus on the role of ovarian surgery in treatment of PCO?
Ovarian wedge resection Stein and Leventhalsuggested ovarian wedge resection (1935). The operation carries considerable risk of adhesion and mechanical infertility (Weinstein and Polishuk 1975)
Laparoscopic drilling versus FSH ovulation induction (Meta-analysis) Farquhar et al 2005 There was no evidence of a difference in the life birth rate between both arms. There was marked reduction in multiple pregnancy rate in ovarian drilling. There are ongoing concern about long term effects of ovarian diathermy on ovarian function and possible peritubal adhesions.
Ovarian diathermy • In a prospective randomized study, of unilateral ovarian diathermy resulted in ovulation in both ovaries, mechanism of action is via correction of disturbed ovarian-pituitary feedback. (Balen and Jacobs 1994)
Types of ovarian surgery for PCOS • Classical wedge resection (Stein and Leventhal 1935). • Laparoscopic wedge resection (Duleba et al 2003). • Ovarian wedge resection by microsurgery via mini-laparotomy (Yildirim et al 2003). • Multiple ovarian biopcies (ref ..) • Ovarian electrocautery (Alborzi 1994). • Ovarian laser vaporization (Asada et al 200)
A prospective dose-finding study of amount of thermal energy required for laparoscopic diathermy • 30 patients were treated by a standard amount of energy at 150 J/ puncture The clinical response to ovarian diathermy seems to be dose dependent.
Ovarian diathermy resulted in adhesions (Mhatre et al 2007) Reduced ovarian reserve and ovarian failure (Api 2009)
We do not have studies to say exactly How many punctures How deep is the puncture Amount of energy used. For how many seconds.