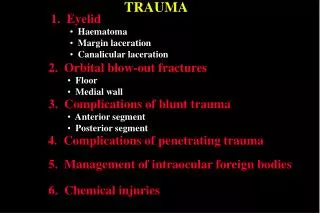
TRAUMA
TRAUMA. Doctor Liang Department of Emergency Surgery, the First Affiliated Hospital, School of Medicine, Zhejiang University. outline. Trauma background definition calssification three peaks of death


TRAUMA
E N D
Presentation Transcript
TRAUMA Doctor Liang Department of Emergency Surgery, the First Affiliated Hospital, School of Medicine, Zhejiang University
outline Trauma background definition calssification three peaks of death trauma system primary survey prehospital--BTLS A B C D trauma center hospital—E.D. principle ATLS procedure DCS+ICU skills Addition (traumatic shock/scores/abdominal trauma)
background • Accidental trauma: the leading cause of death in USA in the 1-to 44-year-old age group and the fourth leading cause overall. (National Center for Health Statistics) • Approximately 10% of total medical spending
Definition • Destruction of organizational structures caused by injury factors including physical factors (such as mechanical force,high fever, electric shock, etc.), chemical factors (such as acids, alkalis and blister agents, etc.) and biological factors (such as insects, snakes, rabid dog, etc.) • Usually referred to the destruction and dysfunction of organizational structures caused by mechanical factors.
Classification-1 According to the integrity of skin Closed traumas Contusion crush injury sprain injury closed fracture concussion injury Open traumas penetrating laceration scrape incised wound
Classification-2 • According to the injury position • head, face, neck • chest • abdomen • pelvis • limbs • multiple injury
In clinic • multiple injury One factor >two anatomic parts injury • Compound injury • >two factors
Three peaks of death after trauma Third peak First peak Second peak minutes~hours Epidural hematoma /Subdural hematoma/ hemopneumothorax /rupture of liver and spleen/pelvic fracture/ massive blood loss Seconds~minutes Brain/brainstem/ spine/heart/aorta/ great vessels injury days~weeks severe inflammation MODS and MOF
Gold time • Gold time = one hours after trauma • Life=emergency
outline Trauma background definition calssification three peaks of death trauma system primary survey prehospital--BTLS A B C D trauma center hospital—ED principle ATLS procedure DCS+ICU skills
Trauma system transport field first aid Trauma system Training& database hospital remedy Prophylaxis system Treatment& rehabilitative
Prehospital • 120 • Airway & CPR • antishock & hemostasis • Simple fixation • life sign monitoring • transport record:time , place, mechanism, and history
Primary survey • minimal trauma: require no testing • moderate trauma: complete blood count, basic metabolic panel, blood type and screen, urinalysis • vital sign instability without obvious source, it is prudent to evaluate the abdomen for hemorrhage
ED(Emergence Department) • Trauma center (Emergency Department): • Ancillary staffing, experienced nurse • Up-to-date technology • Readily available consultants , have advanced skills • Rapid operating room capability • Intensive care unit (ICU) capability • Rehabilitative care
ATLS • ATLS: advanced trauma life support
ATLS principle-1 • 1.Patient life-threatening injured first in group injurys, life-threatening priority of multiple injury • 2.Effective treatment not be delayed without clear diagnosis • 3.Comprehensive analysis of injuries is in need, history in the first assessment, diagnosis and treatment is not necessary.
ATLS principle-2 • If the injured patients and the severity do not exceed the processing power of the medical staff, to give priority to those critically ill, multiple trauma patients. • If exceed, to give priority to those time-consuming short, less manpower and equipment needed to care for patients.
ATLS procedure ATLS assessment Auxiliary examination of second time Life sign monitoring &treatment Specialist treatment prepare Triage first survey Resuscitation &first aid Auxiliary examination of first time
E.D. evaluation • Emphasis on airway, breathing, and circulation (ABCs) • Assessment of airway patency, adequacy of ventilation (respiratory excursion and lung auscultation), hemodynamic status (pulse rate, central and peripheral pulse quality, blood pressure), and evidence of controllable hemorrhage should be immediately linked with interventions.
Crash plan C cardiac P pelvis R respiratory L limb CRASH PLAN A abdomen A arteries spine S nerves N H head
interventions • 1. secure the airway while protecting the cervical spine • 2. enhance oxygenation • 3. provide ventilatory assistance • 4. limit further hemorrhage • 5. gain intravenous access • 6. initiate volume replacement • 7. obtain blood for laboratory and blood bank testing
Important process • 1. Monitoring of heart rate, respiratory rate, blood pressure, temperature, pulse oximetry • 2. Early placement of central venous pressure lines • 3. Placement of a nasogastric or orogastric tube for decompression • 4. Placement of a urinary drainage catheter
Laboratory • Complete blood count (CBC) • Arterial blood gases (base deficit) • Electrolytes (including BUN, creatinine, glucose) • Coagulation studies (PT, PTT, platelet count) • Type and crossmatch for 4 units of blood • Toxicologic studies (as indicated) • Serum lactate • Urinalysis
Radiographs • X-ray of chest, cervical spine, pelvis • CT • US
Skills:Trauma airway management • Expert management of the airway is an essential skill for the emergency physician (EP). • Trauma patients benefit from early control of the airway to ensure adequate oxygenation and ventilation and to protect against aspiration.
Techniques of airway management • orotracheal intubation (OTI) conjunction with rapid sequence induction (RSI) is the preferred approach to the airway management of the majority of patients with traumatic injuries. • blind nasotracheal intubation (NTI) • surgical cricothyrotomy
ED management • 1. Oxygen should be administered to all major trauma patients, early control of the airway may be lifesaving and should take priority over all other interventions. • 2.Gaining intraveneous access rapidly is essential to begin volume replacement and support the hemodynamics.
ED management • 3. Fluid therapy, intravascular volume replacement to compensate for blood loss and restore tissue perfusion has been accepted standard therapy for many years. • Optimal type of fluid: crystalloid solutions such as normal saline Lactated Ringer solution • Fluids may be warmed ahead of time or be administered through a fluid warmer.
ED management • 4. Red blood cell substitutes, withthe ability to carry oxygen • Typed and cross-matched PRBCare the best choice for blood transfusion • If there is ongoing massive hemorrhage, fresh frozen plasma (FFP) and plateletsmay be needed to restore the coagulation system.
ED management • 5. Pneumothorax or hemothorax should be managed by the placement of a large chest tube (32 or 36 French) in the lateral chest.
A B
ED management • 6. A pericardiocentesis needle is inserted in the left subxiphoid area and directed 45 degrees toward the left shoulder or sternal notch in pericardial tamponade patients.