
Dementia
Dementia. Dementia. Progressive deterioration of intellect, behavior and personality as a consequence of diffuse disease of the brain hemispheres, maximally affecting the cerebral cortex and hippocampus. Dementia is a symptom of disease rather than a single disease entity!!!.

Dementia
E N D
Presentation Transcript
Dementia Progressive deterioration of intellect, behavior and personality as a consequence of diffuse disease of the brain hemispheres, maximally affecting the cerebral cortex and hippocampus. Dementia is a symptom of disease rather than a single disease entity!!!
Memory must be impaired to make the diagnosis of dementia. • Loss of memory for recent events is the earlist feature of dementia. • Subsequent symptoms include abnormal behavior, loss of intellect, mood changes, and difficulty coping with ordinary routes. • Insight may be retained initially, but is then usually lost. • Ultimately, there is loss of self-care, wandering, incontinence, and often paranoia.
Dementia has to be distinguished from delirium which is an acute disturbance of cerebral function with impaired conscious level, hallucinations and autonomic overactivity as a consequence of toxic, metabolic or infective conditions. Depression can mimic the initial phases of dementia and it is termed ’pseudodementia’ (which is amenable to antidepressant medication).
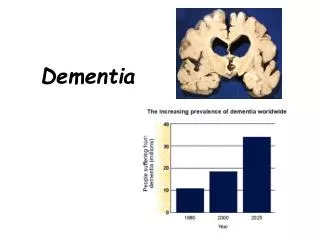
Dementia may occur at any age but is more common in the elderly, accounting for 40% of long-term psychiatric in-patients over the age of 65 years. The prevalence in persons aged between 50 and 70 years is about 1% and in those approaching 90 years reaches 50%. An annual incidence rate is 190/100 000 persons.
Clinical course: The rate of progression depends upon the underlying cause. The duration of history helps establish the cause of dementia: Alzheimer‘s disease is slowly progressive over years, whereas encephalitis may be rapid over weeks. Dementia due to cerebrovascular disease appears to occur ’stroke by stroke‘.
Dementias – classificationBased on cause • Alzheimer‘s disease (~60% of all dementias) • Cerebrovascular (multiinfarct state, subcortical small vessel, amyloid angiopathy,…) (~20%) • Neurodegenerative (DLB, Pick‘s disease, Huntington‘s chorea, Parkinson‘s disease) • Infectious (Creutzfeld-Jakob disease, HIV infection, progressive multifocal leucoencephalopathy) • Normal pressure hydrocephalusTREATABLE! • Nutritional (thiamine deficiency in alcoholics!, B12 deficiency, folate deficiency) • Metabolic (hepatic disease, thyroid d., parathyroid d., Cushing‘s syndrome) • Chronic inflammatory (MS, …) • Trauma (head injury, ’Punch drunk‘ syndrome) • Tumour (e.g. subfrontal meningioma)
Dementias – history and clinical examination • When obtaining a history from a demented person and relative, establish: rate of intellectual decline, impairment of social function, general health and relevant disorders (e.g. stroke, head injury), nutrition status, drug history, family history of dementia. • Tests to assess intellectual function are designed to check: memory, abstract thought, judgement, specific focal cortical functions. The Mini Mental State Examination (MMSE) • On neurological examination note: focal signs, involuntary movements, pseudobulbar signs, gait disorder.
Dementias – further investigation • Blood tests (to exclude hypothyroidism, vitamin B12, thiamine and folate deficiency, Lyme disease, HIV infection, metabolic disorders and inflammatory diseases). • Cranial imaging (CT or/and MRI) (tu, NPH) • PET and SPECT? • EEG (slowing in AD, normal in pseudodementia, periodic complexes in CJD) • Genetic testing (rarely – Huntington mutation, apolipoprotein E4 mutation in AD) • Brain biopsy (if treatable cause is suspected)
Alzheimer's disease • The commonest cause of dementia. • The disorder rarely occurs under the age of 45 years. • The incidence increases with age. • The cause of AD is not known (neurodegenerative d.). • Up to 30% of cases are familial (the loci were found on chromosome 21 and 19). • Pathology – the presence of senile plaques and neurofibrillary tangles in the brain. • Diagnosis of AD may be established during life by early memory failure, slow progression and exclusion of other causes.
Alzheimer's disease • CT scanning aids diagnosis by excluding multiple infarction or a mass lesion. • MRI shows bilateral temporal lobe atrophy. • SPECT usually shows temporoparietal hypoperfusion.
Alzheimer's disease - treatment - Acetylcholinesterase inhibitors (Donepezil [Aricept], Rivastigmine [Exelon], Galantamine [Reminyl]) have been shown to enhance cognitive performance in early disease. Memantine [Ebixa, Axura, Namenda] is approved for moderate disease. However they do not cure! • Treat concurrent depression, anxiety and sleep disorders. Neuroleptic use may be required for behavioral disturbance. • Mangement of AD requires careful advice and counseling of the patient and family and shared care involving the family, caregivers, GPs, hospital specialist, and community psychiatric services. • Long-term residential care is ofte required.
Multi-infarct dementia (MID) • This is an overdiagnosed condition which accounts for less than 10% of cases of dementia. • MID is caused by multiple strokes - SILENT STROKES • Dementia occurs ’stroke by stroke‘, with progressive focal loss of function. • Clinical features of stroke profile – hypertension, diabetes, etc. – are present. More often in males. • Diagnosis is obtained from the history and confirmed by CT or MRI scan (the presence of multiple areas of infarction). • Treatment: Maintain adequate blood pressure control, anti-platelet aggregants (aspirin).
Frontotemporal dementia (Pick's disease) • This progressive condition accounts for 5% of all dementias. • Usually sporadic, it more commonly affect women between 40 and 60 years. • Personality and behaviour are initially more affected than memory. • Frontal lobe dysfunction predominates with apathy, lack of initiative and personality changes. • CT or MRI scans show frontal (and/or temporal) atrophy, often asymmetrical. • SPECT reveal anterior hypoperfusion, EEG is usually normal. • The disorder is characterized pathologically by argyrophylic inclusion bodies within the cytoplasm of cells of the frontotemporal cortex. • There is no treatment, death occuring within 2-3 years of the onset.
Primary progressive aphasia • This condition is one of a group of disorders characterized by asymmetrical cortical degeneration. • Dominant hemisphere perisylvian atrophy is associated with loss of language, which, after many years, becomes a more widespread dementia. • Pathologically non-specific cell loss, Pick’s pathology or spongiform changes are described. • MRI and SPECT confirm focal changes.
Dementia with Lewy bodies (DLB) • One of the most common types of progressive dementia. • Progressive cognitive decline, combined with three additional defining features: (1) pronounced “fluctuations” in alertness and attention; (2) recurrent visual hallucinations, and (3) parkinsonian motor symptoms, such as rigidity and the loss of spontaneous movement. • The symptoms of DLB are caused by the build-up of Lewy bodies – accumulated bits of alpha-synuclein protein - inside the nuclei of neurons in areas of the brain that control particular aspects of memory and motor control. Lewy bodies are often also found in the brains of people with Parkinson's and Alzheimer’s diseases.These findings suggest that either DLB is related to these other causes of dementia or that an individual can have both diseases at the same time. • DLB usually occurs sporadically, in people with no known family history of the disease. However, rare familial cases have occasionally been reported.
Normal pressure hydrocephalus = term applied to the triad of: • Dementia • Gait disturbance • Urinary incontinence occuring in conjunction with hydrocephalus and normal CSF pressure. Two types: • NPH with a preceding cause (SAH, meningitis, trauma, radiation-induced). • NPH with no known preceding cause – idiopathic (50%).
Normal pressure hydrocephalus Aetiology is unclear. It is presumed that at some preceding period, impedence to normal SCF flow causes raised intraventricular pressure and ventricular dilatation. Compensatory mechanisms permit a reduction in CSF pressure yet the ventricular dilatation persists and causes symptoms.
Normal pressure hydrocephalus Diagnosis is based on clinical picture plus CT scan/MRI evidence of ventricular enlargement. NPH must be differentiated from pts whose ventricular enlargement is merely the result of shrinkage of the surrounding brain, e.g. AD. These pts do not respond to CSF shunting, whereas a proportion of NPH pts (but not all) show a definitive improvement with ventriculo-peritoneal shunting.
AIDS dementia complex • Approximately two-thirds of persons with AIDS develop dementia, mostly due to AIDS dementia complex. • In some patients HIV is found in the CNS at postmortem. In others an immune mechanism or an unidentified pathogen is blamed. • Dementia is initially of a "subcortical " type. • CT - atrophy; MRI - increased T2 signal from white matter. • Treatment with Zidovudine (AZT) halts and partially revers neuropsychological deficit.
Trauma • Reduction of intellectual function is common after severe head injury. • Chronic subdural haematoma can also present as progressive dementia, especially in the elderly. • Punch-drunk encephalopathy (dementia pugilistica) is the cumulative result of repeated cerebral trauma. It occurs in both amateur and professional boxers and it manifests by dysarthria, ataxia and expy signs associated with ’subcortical‘ dementia. There is no treatment for this progressive syndrome.
Tumour • Dementia rarely may be due to intracranial tumour, especially when tumours occur in certain anatomical sites. • Mental or behavioral changes occur in 50-70% of all brain tumours as distinct from dementia which is associated with frontal lobe tumours, III ventricle tumours and corpus callosum tumours. • Cognitive impairment also occurs as a non metastatic complication of systemic malignancy.
Mild cognitive impairment (MCI) • MCI is a relatively recent term, used to describe people who have some problems with their memory but do not actually have dementia. • Some people (80%?) will be in the early stages of Alzheimer’s disease or another dementia. Others, however, will have MCI as a result of stress, anxiety, depression, physical illness or just an ‘off day’. • It is estimated that 15% of the population may be experiencing MCI. • Currently extensive research on MCI is ongoing. • At the moment there is not enough evidence to recommend any specific treatments.





















