Diagnosis
Diagnosis. Algorithm for managing Acute Pancreatitis. CONFIRMATION OF DIAGNOSIS (Clinical symptoms, Lipase/Amylase, Ultrasound). ASSESSMENT OF SEVERITY (Clinical Signs, Scoring Systems, Biochemical Markers, contrast CT scan). MILD. SEVERE. ICU. antibiotics. FNA. improve.

Diagnosis
E N D
Presentation Transcript
Algorithm for managing Acute Pancreatitis CONFIRMATION OF DIAGNOSIS (Clinical symptoms, Lipase/Amylase, Ultrasound) ASSESSMENT OF SEVERITY (Clinical Signs, Scoring Systems, Biochemical Markers, contrast CT scan) MILD SEVERE ICU antibiotics FNA improve Supportive care Infection Sepsis Surgical debridement
CONFIRMATION OF DIAGNOSIS CLINICAL SYMPTOMS AND HISTORY SEVERE ABDOMINAL PAIN NON-ALCOHOLIC
History and PE • Severe pain, following a substantial meal • Vomiting does not relieve pain • Epigastric pain • Knifing or boring through the back • Relieved with leaning forward • Tachycardia, tachypnea hypotension, hyperthermia • Temp: mildly elevated • Involuntary guarding over epigastric area • Bowel sounds are decreased or absent
Laboratory tests – on admission Normal Values Patient’s Results CBC Hgb: 130g/dl WBC: 16,000/cumm PMN: 75% Serum amylase: 850 units FBS: 120 mg/dl Serum ALP: 250 IU Serum Creatinine: 1.3 mg/dl Serum Sodium: 145 meq/L Serum Potassium: 4 meq/L Serum Calcium: 9 mg/dl • CBC • Hgb: 120-160 g/dl • WBC: 5,000-10,000/cumm • PMN: 60-70% • Serum amylase: 60-180 units • FBS: 70-110 mg/dl • Serum ALP: 9-35 IU • Serum Creatinine: 0.5-1.2 mg/dl • Serum Sodium: 135-145 meq/L • Serum Potassium: 3.5-5 meq/L • Serum Calcium: 8.5-11 mg/dl
Laboratory tests – on admission Normal Values Patient’s Results ABG PaO2: 90 mmHg PaCO2: 38 mmHg pH: 7.4 HCO3: 20 Serum Bilirubin TB: 2.0 mg% DB: 1.5 mg% IB: 0.5 mg% • ABG • PaO2: 90 mmHg • PaCO2: 35-45 mmHg • pH: 7.35-7.45 • HCO3: 22-26 • Serum Bilirubin • TB: 0.2-1.0 mg% • DB: 0-0.2 mg% • IB: 0-0.8 mg%
Laboratory tests – 3rd hospital day Normal Values Patient’s Results CBC Hgb: 130g/dl Hct: 40% WBC: 19,000/cumm PMN: 80% Serum amylase: 800 units Serum Sodium: 145 meq/L Serum Potassium: 3 meq/L Serum Calcium: 5 mg/dl • CBC • Hgb: 120-160 g/dl • Hct: (Adult males) 42%-54% • WBC: 5,000-10,000/cumm • PMN: 60-70% • Serum amylase: 60-180 units • Serum Sodium: 135-145 meq/L • Serum Potassium: 3.5-5 meq/L • Serum Calcium: 8.5-11 mg/dl
Laboratory tests – 3rd hospital day Normal Values Patient’s Results ABG PaO2: 95 mmHg @ 5L O2 inhalation PaCO2: 40 mmHg pH: 7.2 HCO3: 15 meq • ABG • PaO2: 90 mmHg • PaCO2: 35-45 mmHg • pH: 7.35-7.45 • HCO3: 22-26 meq
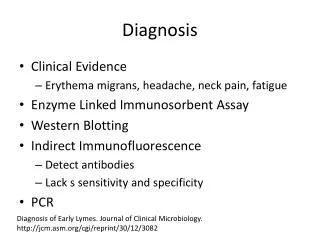
Serum Markers • Elevated because inflammation of pancreas pancreatic acinar cells synthesize, store and secrete a large number of digestive enzyme • LIPASE • Serum indicator of highest probablity of disease • AMYLASE • Increase almost immediately with onset and peak w/in hours • Remain elevated for 3-5 days • No correlation between magnitude of amylase elevation and disease severity • False (+): small bowel obstruction, Perforated ulcer, intraabdominal inflammatory condition • Can also be false (-) in pancreatitis
Radiographic Procedures • CT Scan - “gold standard” • Ultrasonography – presence of gallstones • Endoscopic Ultrasound • ERCP
Computed Tomography Scan • CT scan is more commonly used to diagnose pancreatitis • Gold standard for detecting and assessing severity of pancreatitis • CT scan findings: • mild: interstitial edema • Microcirculation of pancreas remain intact • uniform enhancement • Necrotizing: • Microcirculation of pancreas is disrupted • Gland enhancement is decreased • infected necrosis/pancreatic abscess: associated with necrosis and presence of air bubbles
Ultrasound • Best way to confirm gallstone • Detects: • extrapancreatic ductal dilatation • Pancreatic edema, swelling • Peripancreatic fluid collection • US RESULT: • Liver normal • Gallbladder with multiple stones;wall not thickened • CBD 0.8 cm • Pancreas not visualized GYG
ERCP • Early ERCP (endoscopic retrograde cholangiopancreatography), performed within 24 hours of presentation, is known to reduce morbidity and mortality. • The indications for early ERCP are as follows : • Clinical deterioration or lack of improvement after 24 hours • Detection of common bile duct stones or dilated intrahepatic or extrahepatic ducts on CT abdomen • The disadvantages of ERCP are as follows : • ERCP precipitates pancreatitis, and can introduce infection to sterile pancreatitis • The inherent risks of ERCP i.e. bleeding • It is worth noting that ERCP itself can be a cause of pancreatitis.
Assessment of Severity • Early prognostic signs - Ranson’s Criteria - APACHE II • CT scan findings
Patient – 3rd day hospital admission Base deficit = 7 meq/L Serum calcium = 5 mg/dl Ranson’s Base deficit = 5 meq/L Serum Ca < 8 mg/dl Ranson’s Criteria – acute gallstone pancreatitis
Early Prognostic Signs • Prognostic Implications of Ranson’s Criteria:
Apache II score Age in years History of severe organ insufficiency or immunocompromised Rectal Temperature (Celsius) Mean arterial pressure (mmHg) Heart rate (ventricular response) Respiratory Rate (non-ventilated or ventilated) Oxygenation (use PaO2 if FiO2 < 50%, otherwise use A-a gradient) Arterial pH Serum sodium (mMol/L) Serum potassium (mMol/L) Serum Creatinine (mg/100 mL) Hematocrit (%) White blood count (total/cubic mm in 1000's) 15 minus the Glasgow Coma
APACHE II Score Interpretation 0-4 ~4% death rate 5-9 ~8% death rate 10-14 ~15% death rate 15-19 ~25% death rate 20-24 ~40% death rate 25-29 ~55% death rate 30-34 ~75% death rate over 34 ~85% death rate