Download
1 / 6
60 likes | 186 Vues
Cranial Nerve Clinical Correlations W. Rose 2011. Cranial Nerve Testing http://library.med.utah.edu/neurologicexam/html/cranialnerve_abnormal.html Abnormal: “Cranial nerves 3, 4, and 6 versions” 1

E N D
Cranial Nerve Clinical Correlations W. Rose 2011 Department of Kinesiology and Applied Physiology
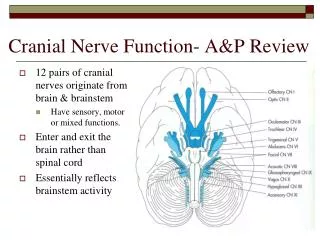
Cranial Nerve Testing • http://library.med.utah.edu/neurologicexam/html/cranialnerve_abnormal.html • Abnormal: “Cranial nerves 3, 4, and 6 versions” 1 • Versions: binocular tests, part of a regular exam. Pt. 1 can’t abduct L, i.e. n.6 (L) palsy. Pt.2 limited adduct, elevate, depress L eye, also shows ptosis-+ & dilated pupil, i.e. n.3 (L) palsy. • Movies from the Neurologic Exam and PediNeurologic Exam websites by Paul D. Larsen, M.D., University of Nebraska Medical Center and Suzanne S. Stensaas, Ph.D., University of Utah School of Medicine. Additional materials for Neurologic Exam are drawn from resources provided by Alejandro Stern, Stern Foundation, Buenos Aires, Argentina; Kathleen Digre, M.D., University of Utah; and Daniel Jacobson, M.D., Marshfield Clinic, Wisconsin. Department of Kinesiology and Applied Physiology
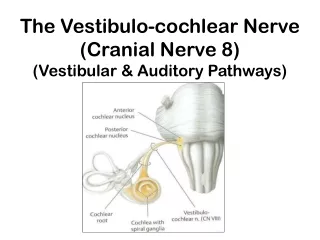
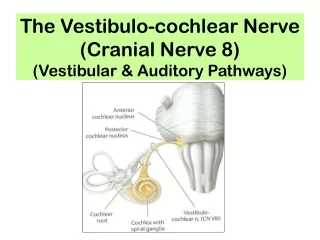
Cranial Nerve Testing http://library.med.utah.edu/neurologicexam/html/cranialnerve_normal.html Normal: “Vestibulo-ocular” (this tests III and VIII) Movies from the Neurologic Exam and PediNeurologic Exam websites by Paul D. Larsen, M.D., University of Nebraska Medical Center and Suzanne S. Stensaas, Ph.D., University of Utah School of Medicine. Additional materials for Neurologic Exam are drawn from resources provided by Alejandro Stern, Stern Foundation, Buenos Aires, Argentina; Kathleen Digre, M.D., University of Utah; and Daniel Jacobson, M.D., Marshfield Clinic, Wisconsin. Department of Kinesiology and Applied Physiology
Cranial Nerve Testing http://library.med.utah.edu/neurologicexam/html/cranialnerve_abnormal.html Abnormal: “Cranial Nerve 12- Motor” 2 If time: Abnormal: “Cranial nerves 3, 4, and 6 ductions” 3 If time: Normal: “Cranial Nerve 12- Motor” 2. Atrophy, weakness, r. deviation of tongue due to lesion of r. cranial nerve 12. 3. Duction (monocular) tests done iff version results abnormal. Pt can’t medially rotate either eye. Observe nystagmus upon abduction of each eye. This & other results (not shown) suggest bilateral internuclear ophthalmoplegia, often caused by demyelinating lesion affecting medial longitudinal fasciculus (MLF) bilaterally. Adduction defect occurs due to disruption of MLF connections between the abducens nucleus and the lower motor neurons in the oculomotor nucleus that innervate the medial rectus muscle. Department of Kinesiology and Applied Physiology
Rash in the ophthalmic distribution of the trigeminal nerve Herpes zoster, Wills and River, NEJM (2010) 362: 1128. See next slide for details Department of Kinesiology and Applied Physiology
Varicella Zoster Virus • Causes chicken pox and later may re-appear as shingles, a.k.a. herpes zoster • Neurotropic: lies dormant for years in dorsal root ganglion neurons • Shingles: painful skin rash, often unilateral and follows dermatome • Member of herpes virus family. Clinically unrelated to cold sores and genital herpes, caused by HSV-1 and HSV-2. Herpes zoster, Wills and River, NEJM (2010) 362: 1128. A previously healthy 57-year-old man presented to the emergency department with 4 days of worsening rash on the left side of his forehead (Panels A and B). He had been seen at a clinic 2 days earlier and started on a course of oral acyclovir. The patient came to the emergency department out of concern about crusting and swelling around his left eye. Vesicular, purulent, and crusted lesions consistent with herpes zoster were evident in the ophthalmic distribution of the trigeminal nerve. Ophthalmic examination with direct visualization, slit lamp, and fluorescein staining showed no evidence of accompanying keratitis or uveitis. The results of laboratory tests, including a complete blood count and comprehensive metabolic panel, were all within normal limits. A test for infection with the human immunodeficiency virus was negative. No underlying immunosuppressive illness or ophthalmic involvement was found, and the diagnosis of herpes zoster was made on the basis of findings from the patient's history and physical examination. The patient completed a 10-day course of oral acyclovir, and clindamycin was added to the regimen for suspected bacterial superinfection. Bacterial culture from the lesions grew methicillin-sensitive Staphylococcus aureus. Six weeks after the initial visit, the rash had resolved but postherpetic neuralgia had developed; it improved slightly after treatment with gabapentin. Department of Kinesiology and Applied Physiology