Renal system lec.no 2 glomerulonephritis
460 likes | 734 Vues
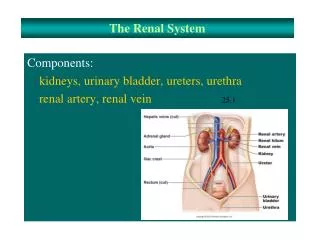
Renal system lec.no 2 glomerulonephritis . Dr:BAKIE.R.R. G lomerulonephritis . Definition: -Inflammation and proliferation of cells within the renal glomerulus which may occur as primary condition or associated with a systemic disorder. The majority of cases are immunologically mediated. .

Renal system lec.no 2 glomerulonephritis
E N D
Presentation Transcript
Renal system lec.no 2glomerulonephritis Dr:BAKIE.R.R
Glomerulonephritis Definition: -Inflammation and proliferation of cells within the renal glomerulus which may occur as primary condition or associated with a systemic disorder. The majority of cases are immunologically mediated.
Pathogenesis Glomerular injury may be the result of : 1- genetic . 2-immunologic . 3- coagulation disorder. Immunologic injury is the most common cause , and results in glomerulonephritis. Evidence of immune mediated glomerular injury includes: 1-morphologic and immunopathologic similarities to experimental immune-mediated glomerulonephritis. 2-The demonstration of immune –reactions in glomeruli. 3-Abnormalities in serum complement and the finding of autoantibodies (anti-GBM) in some of these diseases.
Etiology Primary GN: 1-pos infectious. 2-IGA nephropathy(Berger disease). 3-Membranous. 4-Membranoproliferative. GN associated with Systemic diseases: 1- Vasculitic conditions-Henoch Shonlein purpura, polyarteritis nodosa,SLE and other connective tissue diseases. 2- Infections like SBE, HUS,Shunt nephritis, malaria. 3-Hereditary-Alport’s disease. 4- Others like Diabetes mellitus.
Acute post-infectious GN Acute poststretococcal GN is one of the most common cause of gross haematuria in children . It follows infection of the throat during the cold weather months , and skin infection during warm weather months by certain strains of group A B-hemolytic streptococci.orinfection by other organisms like staphylococci, salmonella, mycoplasma, and viruses.
Pathology and pathogenesis -Morphologic studies and a depression in serum complement level strongly suggested that post streptococcal GN is immune complex mediated. The kidneys appear symmetrically enlarged, all glomeruli appear enlarged and relatively blood less with diffuse mesengial cell proliferation and increase in mesengial matrix. There is deposition of immuno globulin and complement on the glomerular basement membrane.
Clinical features -Post streptococcal GN occur at any age ,but is most common in children aged 5-12 years old. -It occur 1-2wk after streptococcal phrangitis,and 3-6wk after a streptococcal skin infection. -The severity of renal involvement varies from a symptomatic microscopic hematuria with normal renal function to acute renal failure.
Clinical features -Dark “smoky” urine. -Puffy face with fluid retention, usually mild causing only a degree of edema, but when severe can result in heart failure. -Oliguria, in severe cases acute renal failure. -Hypertension, occasionally acute causing encephalopathy and seizures. -Non-specific: malaise, abdominal pain and fever. -The acute phase usually resolves within 1-2 months after onset but urinary abnormalities may persist for more than 1 year.
Investigations -Urinalysis: gross hematuria, granular & RBC cast, and variable proteinuria. -Blood urea and creatinine: are elevated according to the degree of impairment in renal function which may range from minimal to severe. -Electrolytes: show variable degrees of hyperkalemia, hyperphosphatemia, hypocalcaemia and acidosis. Hypocomplementemia ( Low C3 component of complement) -Evidence of recent streptococcal infection: Throat swab, ASO titer, and anti DNase B antibody titer. ASO titer may not rise, particularly after skin infections.
Renal biopsy: usually it is not necessary, should be considered in the following situations: 1-absence of evidence of streptococcal infection. 2-acte renal failure. 3-nephrotic syndrome. 4-normal complement level. 5-persistant gross hematuria for more than 2 months. 6-persistant protein urea for more than 2 months. 7-low level of complement remain for more than 2 months
Management -Acute post-infectious GN is usually mild and requires no specific treatment other than monitoring of daily weight, BP, and fluid balance to limit the risk of fluid overload. -There is no real evidence that bed rest is of benefit. -Salt and fluid restriction can control mild hypertension. ---------Diuretics are helpful if BP is not controlled by salt restriction. -Antihypertensive drugs are needed for more severe cases. -Although it does not seem to alter the course of acute GN, a 10 day course of penicillin is usually given to limit the spread of nephritogenic strains of streptococci. -In few patients the disease is fulminant with rapid progression to renal failure. In such cases dialysis may be needed.
Management-cont. -The child can be discharged home once the renal function is seen to be improving. - Outpatient follow up should continue until urinalysis, BP, and renal function are normal. -Complete recovery occurs in more than 95% of cases, second attacks are rare. -Renal function usually returns to normal within 10-14 days but microscopic hematuria may persist for 1-2 years.
IGA NEPGROPATHY (BERGER NEPHROPATHY) IGA nephropathy is the most common chronic nephropathy world wide. -It is characterized by predominance of IgA within mesaangial deposits in the absent of systemic diseases like SLE. -It is the most common cause of recurrent attacks of gross hematuria.
PATHOLOGY -IGA nephropathy is an immune complex disease that appears to be caused by abnormalities in the IgA immune system. -Familial clustering of cases of this disease suggested importance of genetic factors.
CLINICAL MANIFESTATION -IGA nephropathy is more common in male. -Gross hematuria occur in association with upper respiratory tract or GIT infections. -Loin pain is common. -In some patient there is only microscopic hematuria with or with out protein urea. -It may present with acute nephritc or nephrotic syndrome or combination of both. -Mild to moderate hypertension is often present.
DIAGNOSIS -Recurrent attacks of gross hematuria with or without protein uria which is frequently less than 1gm/24hr. -Positive family history of similar condition. -Normal serum level of C3 in IgA nephropathy helps to distinguish this disorder from post streptococcal GN. -Serum IgA levels have no diagnostic value because they are elevated in only 15% of patients.
-RENAL BIOPSY: shows focal or segmental mesangial proliferation; in some there is generalized mesangial preliferation.IgA is the predominant immunoglobulin deposited in the mesangium.
TREATNENT -The primary treatment is proper control of blood pressure. -Fish oil which contain omega-3 polyunsaturated fatty acid ,decrease the rate of renal progression in adult. -Steroid or other immunosuppressive drugs is of help in some patient. -Angiotensin converting enzyme inhibitors , and angiotensin 2 receptor antagonists are effectives in reducing proteinuria and in retarding the rate of renal progression. -Tonsillectomy may decrease the frequency of hematuria and the rate of renal progression. -Patient with end stage renal disease needs renal transplantation.
PROGNOSIS -Progressive renal injury occur in 20-30% of children at 15-20 years disease onset. -poor prognostic factors are: 1-persistent hypertension. 2-diminished renal function. 3-heavy or prolonged proteinuria. 4-histologica evidence of diffuse mesangial proliferation, glomerular sclerosis,interistetial inflammation and fibrosis.
ALPORT SYNDROME -Is inherited nephritis, caused by mutation in the gene coding for type 4 collagen which is the main component of glomerular basement membrane. INHERITANCE: 1-XLR 85%. 2-AD 5%. 3-AR 10%.
CLINICAL MANIFISTATIONS -All patient wit AS have asymptomatic microscopic hematuria. -Recurrent gross hematuria 1-2 days after an upper respiratory tract infection are seen in 50% of patient. -progressive proteinuria is common by the second decade of life and can be severe enough to cause nephrotic syndrome. -Bilateral sensory neural hearing loss which is never congenital occur in 90% of patient. -Ocular abnormalities include anteriorlenticonuse,corneal erosion.
DIAGNOSIS AS should be suspected in any patient with hematuria with two of the following: 1-GBM thickening or thinning. 2-eyes manifestation like corneal flecks, recurrent corneal erosion, anterior lenticonus is pathognomonic. 3-Sensory neural deafness. -Diagnosis of AS can be done by careful family history ,screening urinalysis of first degree relatives, an audiogram and an ophthalmological examinations.
TREATMENT -no specific treatment is available. -Cyclosporine and angiotensin –converting enzyme inhibitor may decrease the rate of renal progression. -Symptomatic treatment of chronic renal failure is critical like treatment of hypertension ,anemia ,electrolyte imbalance. -Patient with ESRD is treated with dialysis and renal transplantation.
HenochShonleinpurpuraanaphylactoidpurpura Is an IgA mediated vasculitis of small vessels with unknown etiology. Clinical manifestation of the disease: 1-skin manifestation: the skin rash beginning as pinkish maculopapular or urticaria that progress rapidly into clinically palpable petechial and purpuric rash that evolve from red to purple to rusty brown before they fade. The lesions tend to appear in crops on the extensor surfaces of the extremities involving the buttocks. Skin involvement occur in 100% of cases ,but it may be not the initial manifestation. 2-Joint manifestaion:Arthritis occur in more than 2/3 of cases, involve large joints and resolve without sequel.
HenochShonleinpurpura 3-GIT manifestation: Edemaand damage to the GI tract vasculature may lead to intermittent colicky abdominal pain, diarrhea (with or without blood), hematmesis, and rarely intussusception. 4-Renal involvement: occur in 25% of cases, usually as hematuria alone, or hematuria and proteinuria rarely nephroticsyndrome , nephritic syndrome or acute renal failure may occur.Renal manifestations of HSP nephritis occur up to 12wk after the initial presentation of HSP.Chronic kidney disease occur in 2-5% of cases. 5-Rare manifestation:CNS, testicular, eye, and other organ involvement are rare but can be potentially serious.
TREATMENT: Analgesia for pain can be enough, but short course steroids can improve GI and CNS complications.
Hemolytic-Uremic Syndrome Is the most common cause of acute renal failure in young children it is characterized by: 1-Microangiopathic hemolytic anemia. 2-Thrombocytopenia. 3-Renal failure (uremia).
Causes of HUS 1-in 80% of cases of HUS it is presided by gastroenteritis due to Escherichia coli serotype O157:H7 in developed countries. The source of this bacteria is usually undercooked meat or unpasteurized milk especially hamburger. 2-It may also occur after infection by other microorganism like Salmonella,Campylobater, Streptococcus pneumoniae ,influenza, varicella, Epistine-Barr viruse. 3-the causes may be drug like oral contraceptive, cyclosporine. 4-rearly it may be familial inherited autosomal dominant or autosomal recessive. Familial cases are usually not associated with diarrhea.
Pathology and pathogenesis -The primary event is capillary and arteriolar endothelial cell injury that lead to mechanical damage of RBC,platelet adhesion and damage. -intra renal vascular damage lead to cortical necrosis and acute renal failure. The glomerular changes include thickening of capillary walls, narrowing of the lumens and widening of the mesangium.
CLINICAL MANIFESTATIONS -It is more common in children younger than 4 years of age. -Initially the patient has watery or bloody diarrhea with fever ,vomiting ,abdominal pain. -Less commonly patient may presents after upper respiratory tract infections. -After (5-10) days the patient develop hemolytic anemia, thrombocytopenia and renal failure.
DIAGNOSIS -Blood examinations shows hemolytic anemia,reticulocytosis,throbocytopenia,there are helmet cells, burr cells, and fragmented RBC. -there is leukocytosis.WBC count may exceed 30,000/mm2. -Coombs test is negative. -blood urea and serum creatinine are elevated.
Differential diagnosis 1-malignant hypertension. 2-SLE. 3-bilateral renal vein thrombosis.
TREATMENT 1-proper treatment of acute gastroenteritis may prevent development of HUS. 2-in case of gastroenteritis caused by E.coli O157:H7 use of antibiotic should be avoided as it increase risk of HUS. 3-acute renal failure fluid and electrolyte imbalance should be treated aggressively. 4-fresh frozen plasma and plasmapheresis is beneficial in some cases.
PROGNOSIS -With aggressive management of acute renal failure more than 90% survive the acute phase. -Death or end stage renal disease affect 12% of patient . -Poor prognosis is associated with: 1-CNS manifestation like coma,seizures,stroke. 2-WBC counts > 20,000. 3-Ischemic colitis. 4-Hypertension. 5-Dialysis required. -patient with HUS require long term follow up because complications like hypertension ,proteinuria, and chronic renal failure may not be apparent for up to 20 years.
Other causes of glomerulonephritis are: 1-thinglomerularbasement membrane. 2-membranous glomerulonephritis. 3-membranoproliferative glomerulonephritis. 4-GN with SLE. 5-Rapidly progressive GN. 6-Good pasture disease.