Download
1 / 76
770 likes | 1.08k Vues
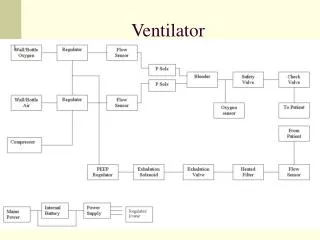
Advanced Ventilator Management Transpulmonary Guided V entilation. Thom Petty BS RRT Lead Clinical Specialist – East CareFusion Critical Care Ventilation. Objectives. Identify the limitations that current Respiratory Mechanics impose upon the management of mechanical ventilation.

E N D
Advanced Ventilator ManagementTranspulmonary Guided Ventilation Thom Petty BS RRTLead Clinical Specialist – East CareFusion Critical Care Ventilation
Objectives • Identify the limitations that current Respiratory Mechanics impose upon the management of mechanical ventilation. • Review the hazards associated with positive pressure ventilation and the sequelae of Ventilator-Induced Lung Injury. • Discuss the role of chest wall, pleura and abdominal pressures during positive pressure ventilation • Introduce the measurement of Transpulmonary Pressure as a valuable ventilation management tool. • Review a Case Study regarding the use of transpulmonary pressures in the management of ventilator settings.
PAO = ( VL / CRS) + ( F x RAW ) PAO= Pressure at the Airway Opening VL= Volume in the Lung CRS= Compliance of the Respiratory System (Lung + Pleura) F= Flow Rate of Gas in L/s RAW = Resistance of the Airway and ETT ( pressure / flow) Mechanics 101: Motion of Air Equation
Pressure in the Airway (Paw) • Measured at the circuit wye • Not the actual pressure in the lungs but the pressure of the entire respiratory system • Reflects both lung and pleural pressures Peri-pulmonary/Pleural Pressure (Pes) • Pressure that is imposed upon the lungs by the Chest Wall and Abdomen • Can be approximated by measuring pressures within the Esophagus Pressure within the Alveoli (Ptp) • The TRUE pressure within the lung • Ptp = Paw – Pes As the Lung Inflates Paw Ptp Pes
Inspiratory Hold • Measures the Plateau Pressure of the entire Respiratory System • Indicator of end-inspiratory lung distension Static Compliance • Reflects the compliance of the entire Respiratory System Expiratory Hold • Measures the amount of intrinsic PEEP of the entire Respiratory System Our Current Respiratory Mechanics Toolbox
What’s so bad about Mechanical Ventilation?
mechanical ventilation can no longer be seen merely as a supportive therapy in ali and ards, but as a treatment modality capable of significantly influencing the course of pulmonary disease and clinical outcome. Viana M, Jornal de Pediatria, 2004 The Hazard that is Mechanical Ventilation
Just what is it that is delivered by the ventilator to the patients’ lungs? • Volume • Flow • Pressure Just What is Positive-Pressure Ventilation?
Adjacent alveoli and terminal bronchioles share common walls • Forces acting on one lung unit are transmitted to those around it (interdependence) • Under conditions of uniform expansion, all lung units will be subject to a similar transpulmonary pressure. • However, if the lung is unevenly expanded, such forces may vary considerably. The Alveolar Structure
Healthy alveoli: • Undergo relatively small changes in size during ventilation unless they totally collapse or re-expand. • Ventilation may occur primarily with changes in the size of the alveolar duct or conformational changes as a result of alveolar folding • Alveoli in ALI: • Undergo large changes in alveolar size • Widespread alveolar recruitment/derecruitment predominate. • Can cause significant shear stress-induced lung injury • Gross tearing of the alveolar wall • Injury to the cell membrane • Ultrastructuralinjury Wilson, J ApplPhysiol, 2001 Carney, CCM, 2005 Steinberg, AJRCCM, 2004 Dynamic Alveolar Mechanics in the Uninjured Lung
Positive-pressure ventilation departs radically from the physiology of breathing spontaneously. • During inhalation positiveintrathoracic pressures are created. • These inspiratory-phase pressures are not homogenously distributed throughout the lung: • Effectively distributed through compliant lung • Flow is attenuated in low-compliant areas • This heterogenocity can result in overdistension of compliant “healthy” lung and underdistension of non-compliant “injured” lung The Problems with Positive-Pressure Ventilation
Early on in the history of positive-pressure ventilation it was recognized that lungs that were ventilated to high pressures have a propensity to develop air leaks. • Thus began the early focus on barotrauma • However, further research has revealed that alveoli that do not overdistend were unlikely to experience injury. • Excessive lung volume (volutrauma) rather than excessive airway pressures produced lung injury. • At the other end of the spectrum, ventilation using low end expiratory volumes that allowed repetitive alveolar opening and collapse (atelectrauma) was also identified as injurious. Whitehead, Thorax, 2002 Diaz, Crit Care Med 2010 The Problems with Positive-Pressure Ventilation
Ventilator-Induced Lung InjuryVolutrauma & Inflammation • Study investigating the release of “Lung Flooding” factors in Rodents ventilated with three modes: • HiP/HiV • High Pressure (45 cmH2O) • High Volume • LoP/HiV • Low Pressure (neg.pres.vent) • High Volume • HiP/LoV • High Pressure (45 cmH2O) • Low Volume (chest bound) Dreyfuss,D ARRD 1988;137:1159
Mechanical and Biochemical in nature • Caused by excessive End-Inspiratory Volumes • Indicated by elevated end-inspiratory (Plateau) pressures • May result from a combination of “Safe” Vt + PEEP • Even “safe” Vt’s may severely over-inflate normal alveoli due to heterogenicity of airflow within the lung • QUESTION: How can a clinician determine if alveoli are over-distended at end-inspiration? Ventilator-Induced Lung InjuryTake-Home Points - Volutrauma
Research has revealed that repeated cyclical collapse & re-expansion of alveoli results in a release of cytokines and the reinforcement and amplification of the local and systemic inflammatory response. • Interleukin-6 • Interleukin-11 • Interleukin-γ • Tissue Necrosis Factor-α Ventilator-Induced Lung InjuryAtelectrauma
Associated with repeated opening and closing of alveoli during ventilatory phasing • Associated with regional differences in ventilation • Worsens surfactant dysfunction • Release of inflammatory mediators into alveolar spaces and into the systemic circulation • QUESTION: How can the clinician determine what PEEP is necessary to keep the alveoli open at end-exhalation Ventilator-Induced Lung InjuryTake-home Points - Atelectrauma
Presumed Mechanism for VILI Mechanical Disruption of Pulmonary Epithelium Mechanotransduction Cell & Tissue Disruption Upregulation & release of Cytokines &, Chemokines Subsequent leucocyte attraction and activation Pulmonary Inflammation: VILI Systemic Spillover: SIRS / MODS MECHANOTRANSDUCTION – Conversion of Mechanical Stimiuls into Chemical Reaction SIRS – systemic inflammatory Response Syndrome MODS – Multi Organ Dysfunction syndrome
1987 - Gattinoni’s CT studies of ALI/ARDS lungs revealed that ALI/ARDS lung is not a stiff organ made up of homogeneously stiff lung units with low static compliance but is a multi-compartmental heterogeneous structure in which there is a portion of aerated normal tissue with normal compliance (baby lung). • Limiting VILI should be accomplished through an Lung Protective approach to ventilator management which includes: • Volume & pressure limitation • Modest PEEP & Plateau pressures • The challenge is to maintain acceptable gas exchange while avoiding harmful mechanical ventilation practices. The need for potentially injurious pressures, volumes, and FiO2’s must be weighed against the benefits of gas exchange support. Lung-Protective Ventilation Theory
There have been six randomized controlled trials evaluating the effect of lung-protective ventilation in comparison with conventional approaches: Lung-Protective Ventilation Research
Tidal Volume Accurately measured The Handful of Ventilator Settings FiO2 Accurately measured Respiratory Rate Accurately measured PEEP Measured but not accurate Plateau Pressure Measured but not accurate
A key limitation to mechanical ventilators is that they report peak airway pressures without distinguishing compliance that reflects intrinsic lung mechanics or chest wall and abdominal pressures Piraino T, Respiratory Care, April 2011 The Problem with Airway Pressures
The Two Settings We Estimate PEEP Measured but not accurate Plateau Pressure Measured but not accurate
Measured at the end of exhalation PEEP is the pressure that is exerted by the volume of gas that is remaining in the lungs (FRC) • Although ventilation with Low Vt’s & Plateau Pressures is generally accepted by the critical-care community, the optimal level of PEEP at which to ventilate remains unclear. • PEEP levels exceeding the “traditional” values of 5-12 cmH2O have been shown to minimize cyclical alveolar collapse and the corresponding shearing injury. • However, potential adverse consequences including circulatory depression and lung overdistensionmay outweigh the benefits • Use of PEEP < 10cmH2O leads to an increase in mortality Amato M., 8th World Congress, Sydney, Australia Dreyfuss, Crit Care Med, 1998 Gattinoni, NEJM, 2006 Muscedere , Am J Respir Crit Care Med. 1994 The Two Settings we Estimate: PEEP
There have been three randomized controlled trials comparing higher versus lower levels of PEEP in ALI/ARDS: • 2010 – Briele Meta-Analysis • Differences in hospital mortality not statically significant • Significant reduction of death in the ICU in the High PEEP group The Two we Estimate: PEEP Research
The Two we Estimate:The PEEP Controversy • Low PEEP/High FiO2 Protocol • FiO2 0.3 0.4 0.4 0.5 0.5 0.6 0.7 0.7 0.7 0.8 0.9 0.9 0.9 1.0 • PEEP 5 5 8 8 10 10 10 12 14 14 14 16 16 18-24 • High PEEP/Low FiO2 Protocol • FiO2 0.3 0.3 0.3 0.3 0.3 0.4 0.4 0.5 0.5 0.5-0.8 0.8 0.9 1.0 1.0 • PEEP 5 8 10 12 14 14 16 16 18 20 22 22 22 24
The Two we Estimate: Optimal PEEP • Ideal PEEP is defined as: • High enough to induce alveolar recruitment, keeping the lung • more aerated at end-exhalation, while not distending “good” • alveoli • Low enough to prevent hemodynamic impairment & • overdistension
The Two we Estimate: Alveolar Recruitability • Briele also suggests that the beneficial impact of reducing intra-tidal alveolar opening and closing by increasing PEEP prevailed over the effects of increasing alveolar distention in ALI/ARDS patients with higher lung recruitability • In ALI/ARDS patients with low potential for recruitment, the resulting over-distension associated with PEEP increases was harmful • How To Determine Lung Recruitability: • Non-Recruitable – If PEEP is and Plateau Pressure then in an equal or greater increment. • Recruitable – If PEEP is and Plateau Pressure then in a lesser increment
The Two We Estimate PEEP Measured but not accurate Plateau Pressure Measured but not accurate
Plateau Pressure is the pressure exerted by the volume of gas in the lungs after an inhalation. • Indicator of “lung fullness” • Plateau Pressure Goal: Keep < 30 cmH2O The Two We Estimate: Plateau Pressure
Check PPLAT (with a minimum 0.5 second inspiratory pause) at least q 4h and after each change in PEEP or VT. • If PPLAT >30 cmH2O: • VT by 1ml/kg to minimum of 4 ml/kg. • If PPLAT < 25 cmH2O and VT< 6 ml/kg: • VT by 1 ml/kg until PPLAT > 25 cmH2O or VT = 6 ml/kg. • If PPLAT < 30 but patient/ventilator dysynchrony is evident: • VT by 1ml/kg to a VT of 7-8 ml/kg if PPLAT remains < 30 cm The Two We Estimate: Plateau Pressure
REMEMBER: Airway pressures displayed by ventilators do not reflect pressures within the lungbut within the Entire Respiratory System • To truly know the pressure within the lung (Transpulmonary Pressure) it is necessary to measure and account for the pressures outside of the lung (Peripulmonary Pressures) • Very difficult to directly measure pressure in the pleura • A number of historic studies have demonstrated reasonable correlation between Esophageal Pressures and Pleural Pressures • Pressure in the pleura adjacent to the esophagus is transmitted to the esophagus. • Pressure within the pleural space is not uniform • Pressure in the dependent & basal regions is greater than in the upper regions of the thoracic cage Solving The Problem with Airway Pressures
Patients on mechanical ventilation are usually supine or semi-recumbent so it is important to account for the effect that mediastinal structures such as the heart have on esophageal pressures. • Washko (2006) and Talmor (2008) have recommended that approximately 2-5 cmH2O be subtracted from the esophageal pressure to more accurately reflect pleural pressures. Solving The Problem with Airway Pressures
Stiff Lung or Stiff Chest Wall? PAW = PTP + PES PAW = PTP + PES 30 = 25 + 5 30 = 15 + 15 Gattinoni, Crit Care, Oct 2004;
How Common are Increased Intra-Abdominal Pressures? Malbrain et al, Intensive Care Med (2004) 30:822–829 13 ICU’s, 6 countries, 97 patients
Can High Intra-abdominal Pressures Really Affect Ventilation? S/P DecompressiveLaparotomy Rigid Abdomen in ACS
To exploit the potential for alveolar recruitment, a transpulmonary pressure that is greater than the opening pressure of the lung must be applied to the lung. • To avoid alveolar collapse after recruitment, a PEEP that is greater than the compressive forces operating on the lung and alveolar ventilation that is sufficient to prevent absorption atelectasis must be provided. • Avoidance of stretch (by maintaining a low plateau pressure) and prevention of cyclic collapse and reopening (by maintaining adequate PEEP and alveolar ventilation) are the physiologic cornerstones of mechanical ventilation in acute lung injury/acute respiratory distress syndrome. Gattinoni et al,CritCareMed2003Vol.31,No.4(Suppl.) Transpulmonary-Guided Ventilation3 Basic Concepts
The Talmor/Ritz Study Survival of ALI/ARDS patients has improved in recent years with the advent of low Vt’s and the use PEEP Optimal level of PEEP is difficult to determine. Could the use of Transpulmonary Pressure Measurements (as estimated by esophageal pressure measurements) enable the clinician to determine a PEEP value that would maintain oxygenation while preventing lung injury due to repeated alveolar collapse and/or overdistention? Mechanically-ventilated ALI/ARDS patients randomly assigned to one of two groups: CONTROL GROUP: PEEP adjusted as per ARDSNet recommendations PES-GUIDED GROUP: PEEP was adjusted to achieve a PTP PEEP of 0 to +10 cmH2O
The Results The primary end point of the study was improvement in oxygenation. Secondary end points respiratory-system compliance & pt outcomes. The study reached its stopping criterion and was terminated after 61 patients had been enrolled. The PaO2/FiO2ratio at 72 hours was 88 mmHg higherin the Pes-group than in the control group This effect was persistent through the 24, 48 & 72 hour follow-up time. Respiratory-system compliance was also significantly improved at 24, 48, and 72 hours in the Pes-guided group
A Sampling of What’s in the Journals • Basing ventilator settings on a maximum allowable airway plateau pressure may leave large portions of the lung under-inflated and at risk of VILI from repeated airway opening and closing. • It is logical that estimating pleural pressures from PES and setting PEEP to achieve a target PTP may allow higher PEEP in many patients without overdistending lung regions that are already recruited.
A Sampling of What’s in the Journals • Systematic use of esophageal manometry has the potential to improve ventilator management in acute respiratory failure by providing more direct assessment of lung distending pressure.
A Sampling of What’s in the Journals • The use of airwayPlateau Pressures to set ventilation may under-ventilate patients with intra-abdominal hypertension and overdistendthe lungs of patients with atelectasis. • Thus PTP must be used to accurately set mechanical ventilation in the critically ill.
A Sampling of What’s in the Journals • Increases in peak airway pressure without a concomitant increase in alveolar distension are unlikely to cause damage. • Critical variable is not PIP but PTP • In patients with a stiff chest wall from non-pulmonary ARDS that may have elevated pleural pressures airway Plateau Pressures may exceed 35 cmH2O without causing alveolar distension
A Sampling of What’s in the Journals • PES can be used to estimate transpulmonary pressures that are consistent with known physiology, and can provide meaningful information, otherwise unavailable, in critically ill patients.
One Hospital’s Protocol for Identification of Pes Candidates • Pplat > 25 cmH2O • Static Lung Compliance < 40 ml/cmH2O • P/F Ratio < 300 • PEEP > 10 cmH2O to maintain SaO2 > 90% • PaCO2 > 60 mmHg or pH < 7.2 attributable to respiratory acidosis • Wolfson Medical Center, Holon, Israel
Esophageal Balloonary: The Catheter • Can utilize either a 5 or 7fr balloon-tipped catheter or a specialized NG/OG catheter that is inserted into the lower third of the esophagus, above the diaphragm. • Pressures that are exerted on the balloon are measured by a transducer either integral in the ventilator or in a separate box • An approximation of proper placement can be made by measuring the distance from the tip of the nose to the bottom of the earlobe and then from the earlobe to the distal tip of the xiphoid process of the sternum.