Download
1 / 86
860 likes | 941 Vues
Learn about the origins, transmitters, receptors, medications, and classifications related to the sympathetic nervous system. Explore adrenoceptors, agonists, mechanisms of action, and pharmacological effects of sympathomimetic drugs.

E N D
Sympathetic Nervous System • Origin • Transmitters • Receptors • Sympathomimetic drugs • Sympathetic Antagonists
Noradrenergic Transmission Classification of Adrenoceptors: -adrenoceptors : Subtypes ( 1&2 ) α1 causes vasoconstriction , mydriasis α2 inhibit insulin & renin release
-adrenoceptors : Subtypes ( 1 , 2 & 3) β1 increases all cardiac properties ,renin & insulin release & lipolysis β2 vasodilation, relax all non vascular smooth muscles, increase liver & muscle glycogenolysis β3inhibit production of leptin
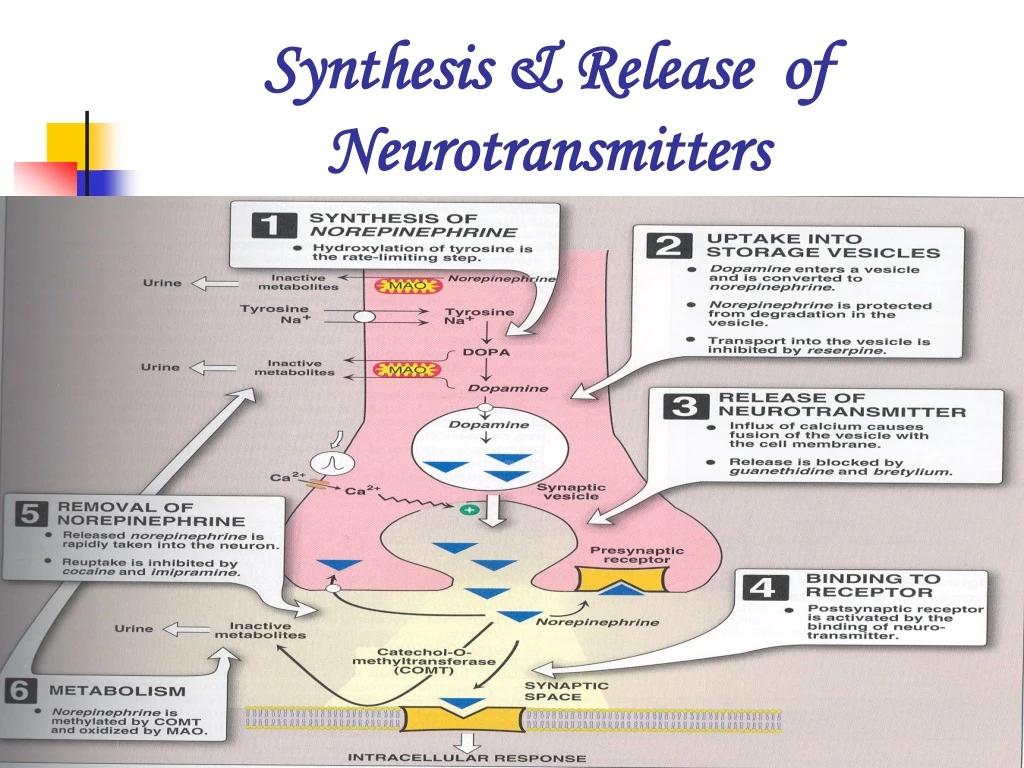
Classification of Adrenoceptor Agonists A: Catecholamines: epinephrine, norepinephrine, isoproterenol & dopamine.
b) inactivation by COMT MAO enzymes inactivate within other tissues as in liver & gut wall. c) Short duration of action. d) Poor penetration into the C.N.S.
Classification of Adrenoceptor Agonists B: Non Catecholamines: • Lacking hydroxyl group. • Long half-life. • Given orally. • . Phenylephrine, ephedrine, amphetamine. • Penetrate better to C.N.S.
Classification According to Mechanism of Action 1- Direct-acting Agonists: e.g.: Epinephrine, norepinephrine, isoproterenol, phenylephrine. 2- Indirect-acting Agonists: Taken up into the presynaptic neuron & cause the release of norepinephrine e.g. amphetamine
3- Mixed-acting Agonists: E.g.: Ephedrine
Pharmacological Actions of Sympathomimetic Drugs 1- CVS: 1 (Heart): Positive inotropic &chronotropic &C.O. Increase oxygen demands on the myocardium.
2 : • Vasodilation of sketal muscles blood vessels. α1- • V.C. of blood vessels in the skin & mucous membranes leading to in mean blood pressure.
2- Eye: 1 : mydriasis. In open-angle glucoma decrease production of aqueous humor by vasoconstriction of the ciliary body blood vessels. .
3- Respiratory Tract: 2 : potent bronchodilator 1: causes vasoconstriction of blood vessels of the upper respiratory tract mucosa decongestion. 4- GIT: Relaxation of GIT S.M through 2 & 2–
5- Exocrine Glands: Regulate secretion of amylase & water from salivary gland, sweat production 6- Metabolic: • 1) β2 : • Hyperglycemia
Release of glucagon • Lipolysis - 2) 2: Decrease insulin release - 3) β3Inhibit the production of leptin by adipose tissue
7- Uterine Smooth Muscle: β2: Delay premature labour through relaxing uterine smooth muscles
8- Genitourinary system α1 :stimulate smooth muscle proliferation in various tissues. E.g.: prostate. β1: stimulate renin secretion α2 : inhibit renin secretion
9- SK.M.: β2 Improve rate & force of contraction used by sport-men to improve performance
10- C.N.S.: Indirect catecholamines have a marked stimulant effect .
Specific Sympathomimetic Drugs Direct Acting: 1- Epinephrine: prototype Stimulates both 1&2 & 1&2 receptors.
Pharmacokinetics - Rapid onset. - Short duration of action. - Given: I.V, S.C, endotracheal tube, inhalation, topically on eye. - Excreted in urine.
Clinical uses 1- Bronchospasm. 2- Anaphylactic shock. 3- Acute asthma (S.C. ). 4- Glaucoma. 2% Topically to reduce I.O.P. in open-angle glaucoma.
5- Cardiac arrest. 6- In anaesthesia with local anaesthetic: a) Increase the duration of L.A. ( by V.C. at the site of injection ). b) Decrease the dose of L.A. c) Decrease the side effects of L.A. d) Control blood oozing of capillary blood ( Local haemostatic effect by V.C. ).
Adverse Effects: 1- C.N.S.: Anxiety, fear, tension, headache, tremor. 2- Hemorrhage: Cerebral hemorrhage as a result of B.P. 3- Cardiac arrhythmias. 4- Hyperglycemia
2- Norepinephrine: - Acts on all types of adrenergic receptors but mainly on α drenoceptors. - Increase peripheral resistance & both systolic & diastolic B.P. - Reflex bradycardia .
Clinical Uses: I.V.I to treat shock
3- Isoproterenol ( Isoprenaline): Stimulates both 1 & 2. 1-Used in atrioventricular block or cardiac arrest. 2- Acute attack of asthma
Adverse Effects: As epinephrine.
4- Dopamine: • Activates α &β adrenoceptors. • D1 & D2 dopaminergic receptors vasodilation
Theraplutic Uses: 1- Shock (I.V.I.) increase B.P & improves blood flow to viscera. 2- Acute heart failure Adverse Effects: Hypertension, arrhythmias, angina.
5- Dobutamine: Selective 1–receptor agonist . Uses: Acute heart failure Adverse Effects:
6- Phenylephrine: - Acts primarily on mainly 1receptors. - V.C. both systolic & diastolic B.P. - Reflex bradycardia .
Topically as nasal decongestant ( produce prolonged vasoconstriction ). Adverse Effects: Hypertensive headache, cardiac irregularities.
7- Clonidine: Is an 2 agonist, used in essential hypertension to lower BP ( action on CNS ). Used to minimize the symptoms of withdrawal from opiates or benzodiazepines .
8- Metaproterenol: - Is not a catecholamines. - Not metabolized by COMT. - Given: orally or by inhalation. - Acts on β1 &β2mainly on 2–receptors. - Used to treat asthma & bronchospasm.
9- Terbutaline: - Short acting 2 agonist. - By inhalation to treat acute asthma. - Produces less cardiac stimulation.
Indirect-Acting Adrenergic Agonists 1- Amphetamine: - Acts on & receptors. - Marked central stimulatory action . a) Attention-deficit hyperactivity disorder of children. b) Narcolepsy(alerting effect &improved attention). c) Appetite control (suppressing effect) as in obesity d) Contraindicated in pregnancy Adverse effects : C.N.S. , Addiction.
2- Methamphetamine: Has a higher CNS effect used as anorexigenic. 3- Tyramine: Found in fermented food as cheese. With MAOI serious vasopressor Effects causing increasing in B.P.
Mixed-Acting Adrenergic Agonists 1- Ephedrine: ( a plant alkaloid ) Indirect & direct acting on & receptors. - Similar to epinephrine but less potent. - Not a catecholamine drug. • Long duration. • C.N.S. stimulant better than epinephrine.
- Absorbed well orally. - Used as prophylactic in chronic asthma.
- Enhances skeletal muscle contractility & improves motor function in myasthenia gravis. - Mild stimulation to CNS alertness, fatigue, insomnia. - Improves athletic performance. - Nasal decongestant. • BP.
Ephedrine (cont.) • Is useful in the treatment of stress incontinence. • Pseudoephedrine(stereoisomerofephedrine) used orally for the relief of nasal congestion. • Less potent than ephedrine in producing tachycardia, hypertension, C.N.S. stimulation. • Used in the treatment of stress incontinence.
Classification of -receptor Antagonists * non-selective e.g. phenoxybenzamine & phentolamine. * 1-selective antagonists e.g. prazosin/ terazosin, doxazosin. * 2-selective antagonists e.g. yohimbine, idazoxan.
Non-Selective - Adrenoceptor Antagonists Phenoxybenzamine: Blocks both 1 and 2 irreversibly . Blocks the action of histamine ,Ach & 5HT. Long-acting (24hrs).
Phentolamine: Produces a competitive blocking of 1 & 2 receptors.-short acting (few hrs). Both drugs cause: 1) Postural hypotension. 2) Reflex tachycardia.
- Increase in C.O. & H.R. ( reflex response to the fall in B.P, mediated through - adrenoceptors, also due to block 2 in heart ).
N.B.: The block of 2–adrenoceptors increase in noradrenaline release which make the drug unsuccessful in maintaining lowered blood pressure.
Therapeutic Uses: 1- Pheochromocytoma. 2- Raynaud,s disease.
Adverse Effects: - Phenoxybenzamine causes postural hypotension, nasal stuffiness, nausea, vomiting, impotence, tachycardia. - Phentolamine: As phenoxybenzamine but more to induce cardiac arrhythmias and anginal pain. Both are contra-indicated in patients with decreased coronary perfusion.
Selective 1- Antagonists Prazosin (short half-life) ,doxazocin& terazocin (long half life )allowing once- daily dosing. 1–antagonists cause vasodilatation & fall in arterial pressure, but less tachycardia than with non- selective blockers.


















