Download

1 / 57
650 likes | 726 Vues
Osteoarthritis of the Knee: Current Management. Goals. To control pain Minimize disability Improve the quality of life prevent progression of the process. Nonpharmacologic Education Weight loss Physical therapy Orthotics Occupational therapy Aerobic exercise Diet. Pharmacologic

E N D
Goals • To control pain • Minimize disability • Improve the quality of life • prevent progression of the process
Nonpharmacologic Education Weight loss Physical therapy Orthotics Occupational therapy Aerobic exercise Diet Pharmacologic Analgesics NSAIDs Topical analgesic Intraarticular Viscosupplementation Aspiration/intraarticular steroids Glucosamine Chondroitin sulfate Diacerin Knee Ost. Management
Patient Education • Physician-patient dialogue • Reading • Other • Internet • Health-Food Store • Talk radio • Television • Word-of-Mouth • Arthritis Foundation-related
OA Development Framingham knee OA study: 12 lbs loss chance (50%) of developing OA in women OA Symptoms 3-6 kg weight loss correlated with knee & hip osteoarthritis scores Walking program: loss of body fat pain Weight Loss
Orthotics • Bracing • Appropriate footwear (eg shock-absorbing insoles) • Lateral-wedged insoles (“antisupinators”) for genu varum
Diet • Vit. C • Vit. E • Vit. D • Beta-caroten
Analgesics • Acetaminophen • Tramadol • Opoids
Acetaminophen • Dosing: 4 gram/day limit • Safe • Hepatotoxicity • Renal failure ?
ADVANTAGES Rapid onset (1 hr) Rapid peak (2 hours) Side effects No GI bleeds No CV side effects Comparable pain relief to Acetaminophen “Non-addictive” Not a controlled medication DISADVANTAGES Qid dosing Inconvenient Peaks & valleys Side effects Dizziness Nausea/vomiting Lowers seizure threshold: (can’t take with certain medications) Not as powerful as pure narcotic analgesics Scant literature in osteoarthritis Tramadol (Ultram)
Topical Analgesics • Indicated as adjunctive treatment or monotherapy for mild-to-moderate knee pain in patients who • Do not respond to acetaminophen & • Do not wish to take systemic therapy • 3 ACR-recognized categories • Capsaicin • Salicylates • NSAIDs
Nonselective NSAIDs • More effective than Acetaminophen • Side effects • Should be avoided in those with peptic ulcer di. , intrinsic renal disease, congestive heart failure, cirrhosis, and volume depletion • May be associated with accelerated joint destruction
COX2 inhibitors • Their efficasy is similar to nonselective NSAIDs • Lower GI toxicity • Cardiovascular adverse events • Withdrawal of two agents, rofecoxib and valdecoxib from the market
INTRAARTICULAR HYALURONANS • Sources of hyaluronate: • Rooster combs • (E coli: new) • A small pain relieving advantage • Side effects: Postinjection flare Hypersensitivity reaction
INTRAARTICULAR GLUCOCORTICOIDS • Indication: in patients who don not respond to NSAIDs, and in patients with inflammatory osteoarthritis in whom NSAIDs are contraindicated • Effect may last 4-6 weeks • Cartilage “Damage” with repeated use
Opioids • ACR Guidelines (2000): • “Patients who do not respond to or can not take tramadol and who continue to have severe pain may be considered candidates for more potent opioid therapy.” • The following may occur: • Tolerance • Dependence • Side effects- esp. constipation {Altman, 2000: pp 9-10}
Glucosamine sulfate • Several but not all controlled human studies have shown a modest decrease in symptoms • May also prevent cartilage loss in established osteoarthritis • Glucosamine, chondroitin sulfate, and the combination of glucosamine and chondroitin sulfate, do not appear to be significantly more efficacious than placebo (Clegg Arthritis Rheum 2005) • Duration
Other drugs • Colchicine • Antimalaria • Diacerin • Tetracyclines
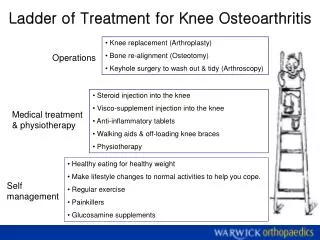
Surgical Therapy • Joint replacement • if “radiographic evidence of joint damage and moderate to severe persistent pain or disability, or both, that is not substantially relieved by an extended course of nonsurgical” (NIH Consensus Conference) • Osteotomy (temporizing) • Cartilage implant (experimental) • Tidal irrigation and debridement not proven
Pathogenesis and management of pain in osteoarthritis Topic review May 19,2005 Sasithorn Chabchaisuk MD.
Introduction • Osteoarthritis is a common disorder of synovial joints. • Strongly age-related, being less common before 40 years,but rising in frequency with age, such that most people older than 70 years have radiological evidence of osteoarthritis in some joints.
The clinical problems associated with pathological and radiographic changes • joint pain related to use • short-lasting inactivity stiffness of joints • pain on movement with a restricted range • cracking of joints (crepitus)
However,correlation between radiographic evidence of osteoarthritis and the symptomatic disease is rather weak. • Should be studying the cause of joint damage, or the causes of pain and physical disability in older people.
Scope • The relations between joint damage and joint pain. • The genetics of osteoarthritis. • The principles of diagnosis, assessment, and management.
1.Joint damage and joint pain • In the 1960s, John Lawrence and colleagues, showed that people with radiographic evidence of osteoarthritis were more likely to have joint pain than were those without any such changes, but also that severe radiographic changes could be present with few or no symptoms.
More recent studies have confirmed and extended that radiographic evidence of joint damage predisposes to joint pain, but the severity of the joint damage on the radiograph bears little relation to the severity of the pain experienced.
Risk factors associated with joint damage andits progression • Age • Family history • Inherited and developmental conditions that affect bone or joint growth or shape • Joint injuries • Selected activities • Obesity the balance of risk factors varies according to joint site.
Risk factors for progressive joint damage some evidence that it different from incident osteoarthritis although the problems with definitions and cut-off points mentioned make it difficult to make this distinction. • Bone density + or –
The pathogenesis of joint damage Articular cartilage. molecular level • gradual proteolytic degradation of the matrix • increased synthesis of the matrix components by the chondrocytes
morphological changes • cartilage surface fibrillation • cleft formation • loss of cartilage volume
Bone :less well understood, • development of osteophytes at the joint margin • ossification of cartilage outgrowths • major changes in the vascularity and turnover of the subchondral bone.
Cytokines and other signalling molecules released from the cartilage, synovium, and bone affect chondrocyte function. • Role for inflammation in osteoarthritis, at least in some patients and in some phases of the disease.
environmental risk factors mentioned mechanical. • Studies have stressed the importance of muscle weakness, joint instability, and malalignment as possible causes of osteoarthritis • Implicit in the concept of osteoarthritis disease modification is the idea that reduction of structural joint damage will translate into symptomatic benefits and improved quality of life. This concept remains unproven.
Risk factors for joint pain few data are available about the risk factors for joint pain. • joint pathology • radiographic changes • various physical activities • psychological wellbeing • health status
The pathogenesis of joint pain • synovitis • subchondral bone changes • peripheral pain sensitisation • central pain sensitisation Finally, the experience of pain will be modulated by psychological, social, and other contextual factors
neurogenic inflammation can contribute to joint damage • inflammation might be an important feature of the process of osteoarthritis. • Pain is accompanied by local production of substance P and cytokines that can interact with inflammation pathways and thereby make a secondary contribution to joint pathology.
2.Phenotypes, genotypes, and classification • Osteoarthritis is a multifactorial disease with genetic and environmental determinants. • All cases are probably affected by both genetics and environment, with a continuous distribution between the extremes of predominantly genetic or predominantly environmental.
Recent reports have identified several chromosomal loci and gene variations associated with an increased risk for osteoarthritis. • coding for molecules in the cartilage matrix such as collagen types II, IX, and XI, COMP, and matrilin-3.
Many but not all genetic variations or mutations are associated with variable expression of the phenotypes spondyloepiphyseal dysplasia (SED) or multiple epiphyseal dysplasia (MED).
Diagnosis and assessment differentiation from • referred pain • periarticular (soft-tissue) conditions • somatisation (regional pain in the absence of any local pathological cause)
Assessment • Radiograph • disease-specific questionnaires • Knee injury and osteoarthritis outcome score” (KOOS) • Western Ontario and McMaster Universities osteoarthritis index (WOMAC)
Principles of management • many elderly people regard musculoskeletal aches and pains and stiffness as a normal part of the aging process, rather than a disease. • Many never seek medical help. • It is important not to overtreat those who do seek help and advice, and that it is inappropriate to medicalise most of those with mild osteoarthritis.