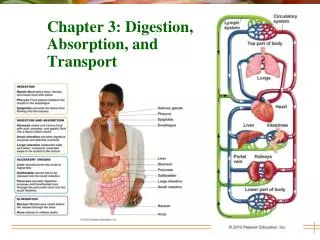
Transport and Function of Blood in the Cardiovascular System
490 likes | 605 Vues
Explore the composition of blood, function of blood cells, the cardiovascular system, cardiac cycle control, factors influencing heart rate, and mechanisms affecting cardiac output and peripheral resistance. Learn about the role of cardiac output in tissue oxygen delivery and myocardial perfusion. Discover how preload, afterload, and contractility impact cardiac function, along with the effects of various drugs on heart rate and blood pressure regulation.

Transport and Function of Blood in the Cardiovascular System
E N D
Presentation Transcript
Link to presentation used in class (supplemented by additional slides…) • Stephen Taylor transport presentation
Syllabus details relating to BLOOD • 6.2.6 State that blood is composed of plasma, erythrocytes, leucocytes (phagocytes and lymphocytes) and platelets • 6.2.7 State that the following are transported by the blood: nutrients, oxygen, carbon dioxide, hormones, antibodies, urea and heat
All cellular components originate from haemopoetic stem cells in the bone marrow
Mammalian 4-chambered hearts develop from 3-chambered hearts
6.2.1: Draw a heart, labelling the 4 chambers, associated blood vessels, valves and route of blood through the heart
Let’s draw a heart! • Drawing a heart...
Control of the cardiac cycle • control of the cardiac cycle • conducrtion system of the heart
Explain the basic cardiac cycle… • Animation 1 • slightly more detailed cardiac cycle
Control of heart rate In order to understand control of heart rate, we need to understand WHY heart rate might increase or decrease…. Give me some reasons why heart rate might increase or decrease?
Heart rate and force of contraction are controlled by the medulla (brainstem) • Cardio-accelerator centre – cardiac nerve: increases heart rate (epinephrine) • Cardio-inhibotorycentre – vagus nerve – decreases heart rate (Ach)
The medulla responds to many factors An increase in carbon dioxide tension in the blood is sensed by chemoreceptors in the heart and carotid artery, and sent to the medulla for processing…
The sino-atrial node is affected by both sympathetic (adrenaline/noradrenaline) and parasympathetic (Ach) fibres
Cardiac output • Cardiac output = volume of blood pumped by the heart in L/minute. • Cardiac output is is the product of HEART RATE (BEATS/MINUTE) and STROKE VOLUME (ML/BEAT) • CO can be increased by means of increasing heart rate OR stroke volume
Tissue oxygen delivery:‘the bottom line’ • depends on cardiac output (cardiac function and forward flow) and arterial oxygen content (CaO2) • Oxygen delivery (DO2) = cardiac output multiplied by the oxygen content of blood DO2= CO X [Hb] X SpO2 X 1.34 (each 1 g of haemoglobin can carry 1.34 g of oxygen)
Myocardial perfusion myocardial perfusion occurs during diastole • A high heart ratemeans less time for diastolic filling and myocardial perfusion • A high heart rate increasesmyocardial work and increases myocardial oxygen requirement: the heart has to work harder’
Cardiac Output (intrinsic ability of heart) Heart Rate Stroke Volume (volume ejected/contraction) (-) Drugs Hypothermia Vagal stim. Symp stim • (+) • Anticholinergics • Symp stim Hyperthermia Preload Afterload Contractility vasopressors Venous blood volume Sympathomimetics Depressant drugs Fluid Therapy
is resistance to blood flow provided by the vascular bed determined principally by vascular tone also affected by blood viscosity and ventricular wall tension arterial blood pressure is the PRODUCT of CO and total peripheral resistance If CO remains the same and afterload then BP rises If CO remains unaltered and afterload (e.g. acepromazine) then BP falls Total peripheral resistance
Heart rate can be influenced by MOST anaesthetic drugs: opioids α2 agonists inhalants ACh inhibitors (anticholinergics) barbiturates ketamine severe bradycardia (not compensated by changes in stroke volume) or severe tachycardia will reduce cardiac output Heart rate may affect cardiac output during anaesthesia
decreased preload (most of filling occurs in first half of diastole) decreased stroke volume decreased myocardial oxygenation potential (coronary arteries fill in diastole) Severe tachycardia decreases cardiac output