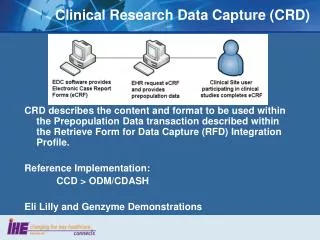
Clinical data capture and communication
300 likes | 519 Vues
Clinical data capture and communication. Prof Jeremy Wyatt AMC, Amsterdam j.c.wyatt@amc.uva.nl. Outline. What is clinical data ? What types of data are there ? Why do we collect it ? Data capture or communication ? How reliable is clinical data ? Causes of data errors

Clinical data capture and communication
E N D
Presentation Transcript
Clinical data capture and communication Prof Jeremy Wyatt AMC, Amsterdam j.c.wyatt@amc.uva.nl
Outline • What is clinical data ? • What types of data are there ? • Why do we collect it ? • Data capture or communication ? • How reliable is clinical data ? • Causes of data errors • How to reduce data errors • Care pathways as a data collection / communication tool
The cycle of clinical information Clinical practice innovation Knowledge assembly Clinical knowledge Libraries, internet, practice guidelines... informs contributes to informs Quality improvement Reminders, audit & feedback... Evidence base Aetiology, genomics, drug effectiveness... Patient management Diagnosis, investigation, therapy, review... improves informs generates builds Patient data Clinical / lab findings, past history, preferences... Research information management Data management
Abstraction Decision Data Evidence Knowledge Strategy Information What we use to make decisions, inform actions Specific to a case: About the world: Raw information More interpreted
Patient data Patient data: information about a patient and their circumstances relevant to clinical decisions, eg. • Demographics: age, gender, occupation… • Symptoms & signs • Past history, medications • Social history: habits, family, living arrangements • Test results, images • Preferences, beliefs, information-seeking habits… • Hypotheses: problems, differential diagnoses… • Actions: what has been tried, done
Forms that patient data can take • Smells • Sounds • Spoken words • Text • Numbers • Drawings • Images – static, moving • 3D solids - palpation
Sources of patient data • Patient themselves • Carer, relative, friend, other informant • Clinician • Laboratory, imaging dept. • Past records • Other professional: social worker, prison officer, teacher…
Data capture methods Patient – questionnaire, diary, forms, touch screen, email, browser, phone menu system, PDA… Clinician – writing, typing, point and click, dictation / transcription, voice recognition Direct signal, image capture and interpretation Text processing – reports, discharge summaries
Reasons for capturing patient data • For immediate clinical decisions: • By yourself • By others (means communicating the data) • For future clinical decisions: • Means memorising or recording the data • For other purposes: • For quality improvement, education • For clinical research • For management / reimbursement • To act as evidence in a court case
report delivery data capture data processing Data capture or communication ? communication
Clinical coding dept. DoH GP Laboratory, imaging dept. Medical secretary PAS, WL system Main patient data flows in a hospital Record library Paper record Operation note Discharge summary Lab reports Clinical notes Outpatient letters Doctor Pharmacy
Problems of electronic clinical data communication • Urgent lab results missed in 45 A&E cases (XXX) • Names of virology tests muddled in GP systems (HepBSag, anti-HBcAg…) • Still cannot transmit a GP record electronically for 20% of patients who change GPs every year (printed out, re-keyed – A. Majid BMJ 2003)
Some sources of data errors • Mis-identification of patient • Patient recall • Elicitation process – training, definitions • Recording process - transcription • Data transmission • Data processing • Data retrieval • Short term memory (JW will say a number – no cheating !) • Data perception • Data interpretation
Data transcription • Typical figure 4% error rate (Norton ’81), 20% of forms need to be clarified • Best studies: 0.2%, 2% queries • No learning over 20 weeks • Errors increase as no. of choices increase • Role of transcribers: • errors varied from 1-10% between transcribers • rates varied from 30-130 records per hour • transcribers with lowest error rates were fastest
Aspects of errors • Frequency • Size of deviation: • How obvious is it • Examples (Gulliford ’93, cancer registries): • Dates of birth: 93% accurate, mean error 1 day • Radiotherapy dose: 84% accurate, mean error 14 Gray [= 1/3 of normal dose]
Does electronic communication help ? Systematic review of 176 Medline-listed reports of structured electronic communication to or by GPs 30 articles eligible: 28 described potential effects, only 5 had objective data Results: • Speed of communication: faster in 4 studies • Content of information and records: improved in 2 studies • Quality of care: improved slightly in 1 study (Branger ’99, shared care for diabetes – slight improvement in HbA1C levels) Conclusion:“The literature provides a disappointingly small number of studies that demonstrate improvement of quality of care by means of electronic communication” Van der Kam, Int J Med Inf 2000; 60: 59-70
Can patient data be safely re-used ? Mrs Smith’s glucose was 7.8mM on 1/2/03 Issues: • Patient ID certain ? • Type of specimen: venous / arterial / capillary blood; urine; CSF; pleural fluid… • Actual value (glucometer calibration, local ref. range, artefact…) • Time taken (fasting / not) • Other context – pregnant; disease presence & stage; therapy at the time; previous values… • Is the data relevant anyway ?
Reliability of clinical data • Is the patient pale / jaundiced ? • Is there a heart murmur ? • Is the patient disorientated ? • Does the patient have signs of bronchitis (COAD) ?
Uncertainty in clinical data Signs of a common disease: COAD McAllister F. Why we need large, simple studies of the clinical examination. Lancet 1999; 354
Solution • Review existing studies, carry out an SR, eg. JAMA Rational Clinical Exam series – CAGE score to detect alcoholism, diagnosis of DVT • Where past studies permit no sound conclusions, develop a protocol and carry out a new large study using the internet – Clinical Assessment of the Reliability of the Examination • See CARE: www.carestudy.com/
Reasons for inaccurate data • Error: “Patients with terminal cancer” who had neither serious illness nor cancer – Rees, BMJ 1987 • System error: • Haste (NAD – not actually done ?) • Missing cases notes – halved mortality in low birthweight babies cf. prospective study (Westgren ’86) • Reimbursement – GPs record procedures on which incentive payments depend (Pringle ’91) • Other: • Pre-surgery renal failure rate in cardiac patients jumped 6 X when NY State published surgeon-specific death rates (Green ’95) • Patient diaries: ¼ of entries more than 6 hours after intended time or invented (Chowienczyck ’94)
Some sources of error Search mis-analysis Lab report poor criteria mis-filing transcription, coding errors Paper record Computer record Patient poor search mis-informing mis-recording Clinical finding Result hard to interpret Inference
Studies on records Compare written record to tape of consultation: • Main complaint: 92% complete • History of present illness: 72% • Other history: 29% • Advice on smoking: 29%
Improving data capture • Problem-specific checklists • Standardised, validated wording and question order • Clear prompts & definitions, space for comments • Direct coding of answers – check boxes, tabular foms (Fries ’74) • Absolute and “verify” range checks; consistency checks across fields; check on legal values • Redundancy: check digits, double keying • Compensation: uppercase only + Soundex algorithm to match names • Make the form the only record & provide incentives to use it – care pathways
Care pathways Problem-specific multi-professional record (for eg. hip replacement, heart attack, stroke) with: • Space to record data, actions, initials • Space to record reasons why data not collected / actions not carried out (“variance tracking”) • Key guideline recommendations, reminders, scoring systems Describe the default course of a patient through the health system, day by day Can share with patients / carers See: www.nelh.nhs.uk/carepathways/
The aim of ICPs To have... • the right people • doing the right things • in the right order • at the right time • in the right place • with the right outcome • all with attention to the patient experience • and to compare planned care with care actually given (NeLH ICP web site)
Further reading Wyatt JC. Acquisition & use of clinical data for audit and research. J Evaluation in Clin Practice 1995; 1: 15-27 Wyatt JC. Clinical data systems series, Lancet 1994: Part I: Data and medical records. Lancet 1994; 344: 1543-47 Part II: Components and techniques. Lancet 1994; 344: 1609-1614 Part III: Developing and evaluating clinical data systems. Lancet 1994; 344: 1682-88